For the millions of couples who have sat in a fertility
clinic waiting room, the math is quietly brutal. You produce embryos. They look
healthy under the microscope. A doctor transfers them to the uterus. And then
nothing. The embryo simply does not implant. No explanation is offered because
until recently, medicine had very little to say about why a viable-looking
blastocyst might silently fail once it's inside the body.
That silence may finally be breaking.
A study published this May in Science Bulletin by
researchers at Tongji University in Shanghai has identified what appears to be
a fundamental molecular error in IVF embryos, one that is present from the very
earliest stages of development and that, if left uncorrected, not only prevents
the embryo from implanting but may quietly program metabolic disease into any
child who does make it to birth.
The discovery centers on a cellular communication pathway
called Wnt signalling, and it raises a possibility that has direct implications
for how IVF embryos are cultured and prepared for transfer.
What the Wnt Pathway Does and Why It Matters
Here
Inside every developing embryo, hundreds of molecular
signals act like switches, telling cells when to divide, when to specialize,
and when to quiet down. Wnt is one of the most ancient and influential of these
signals. It plays a critical role in maintaining the embryo's early,
uncommitted state, a phase called naïve pluripotency, in which cells have not
yet decided what type of tissue they will become.
Here is the crucial point: at the moment of implantation,
the embryo must actively shut off that naïve state and switch into a new mode,
called primed pluripotency, where cells begin differentiating into the tissues
that will form the fetus and placenta. This transition from naïve to primed is
not optional. It is an absolute developmental requirement for successful
implantation.
Wnt signalling, the researchers found, is what governs when
this switch gets thrown. And in IVF embryos, the switch is stuck.
A Flaw Detectable from the First Hours
To study this problem, the team used a mouse model and
built a sophisticated three-dimensional culture system that allowed them to
observe embryo behaviour during the peri-implantation window, the few days
between blastocyst formation and uterine attachment that are ordinarily
invisible to researchers and clinicians alike.
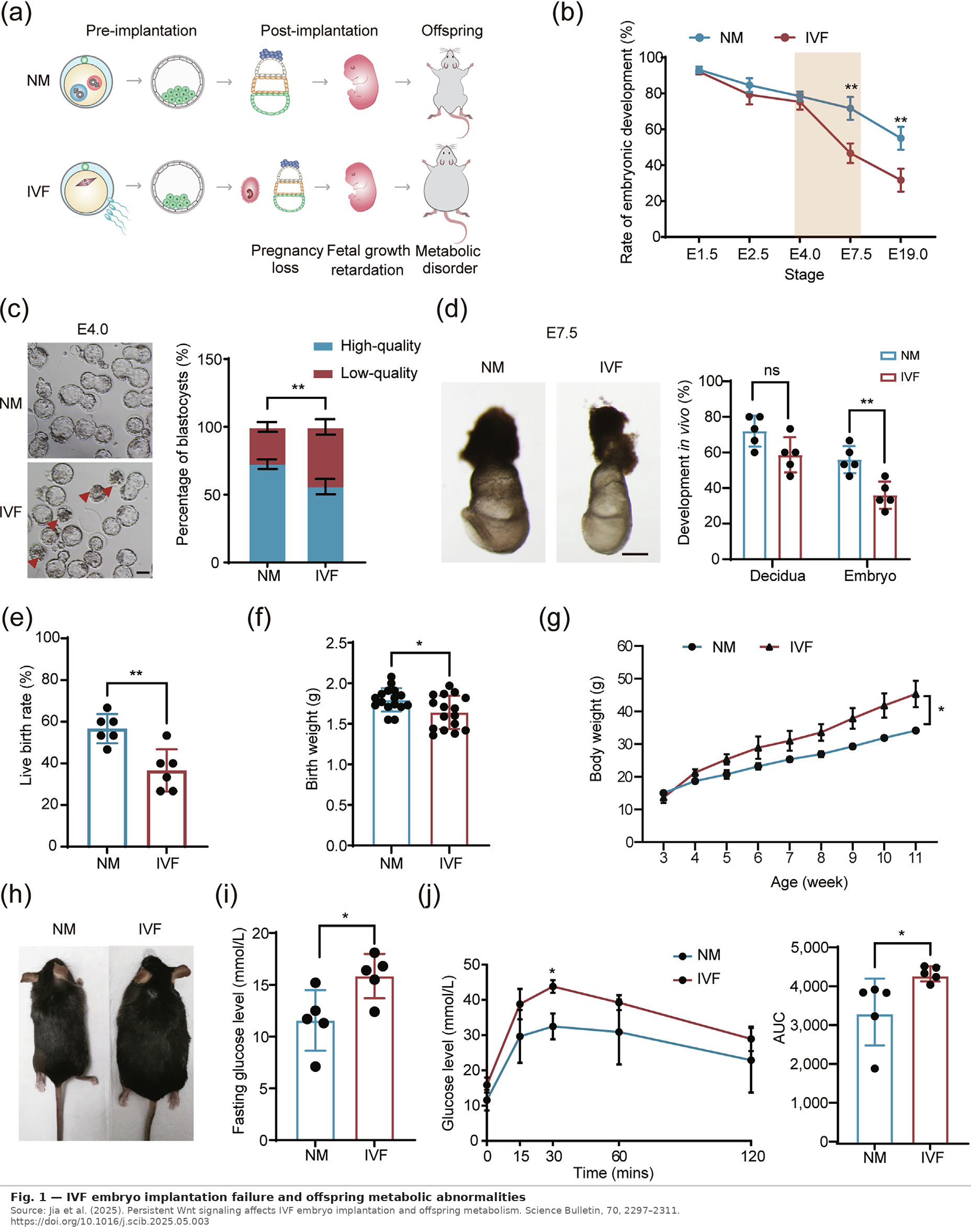
What they found surprised them. When they inserted a
fluorescent reporting system that glows green wherever Wnt signalling is
active, IVF embryos lit up far more brightly than naturally conceived embryos.
At the morula stage, just days after fertilization, well before any embryo is
transferred to a uterus, nearly 46% of IVF embryos were showing abnormal Wnt
activity, compared to about 20% of naturally conceived ones. By the blastocyst
stage, the gap widened further: 62% versus 36%.
This was not a subtle statistical difference. Wnt
signalling was persistently, aberrantly elevated in IVF embryos from the very
beginning.
The reason, it turned out, traced back even further to the
pronuclear stage, essentially the first hours after fertilization. A gene
called Dkk1, which produces a protein that acts as a natural brake on
Wnt signalling, was dramatically underexpressed in IVF embryos. And the cause
of that underexpression was epigenetic: the molecular "marks" that
normally activate the Dkk1 gene were insufficiently established during the IVF
process itself.
In other words, something about oocyte retrieval,
laboratory culture conditions, or in vitro fertilization leaves a molecular
fingerprint on the embryo's genome before it has even divided for the first
time, and that fingerprint suppresses the very gene the embryo needs to
regulate one of its most important developmental signals.
What happens to an Embryo That Cannot Turn Off
Wnt
With Wnt signalling running unchecked, a cascade of
problems follows. The researchers traced these effects using detailed gene
expression analysis and chromatin profiling, essentially reading the molecular
landscape of individual embryonic cells at the moment of implantation.
The epiblast cells in IVF embryos, the cells that will
eventually form the fetus, were stuck in naïve mode. Genes associated with
undifferentiated stem cell identity remained abnormally active. Genes
associated with the primed, implantation-ready state were suppressed. One gene
in particular, Otx2, which is the master coordinator of the
naïve-to-primed transition, was specifically silenced by persistent Wnt
signalling. When the researchers knocked out Otx2 in normal mouse
embryos, those embryos developed the same implantation defects seen in IVF,
confirming that suppressing this one gene was sufficient to reproduce the IVF
phenotype.
The embryos could not organize themselves properly. Under
the microscope, instead of forming the orderly rosette structures that
characterize a healthy peri-implantation epiblast, IVF embryos produced
disorganized, architecturally disrupted tissue. The developmental program had
broken down.
And the consequences extended well beyond implantation.
The Long Shadow: Metabolic Disease in Offspring
The researchers tracked offspring born from IVF embryos
through adulthood, feeding them a high-fat diet to stress their metabolic
systems, a standard method for revealing hidden physiological vulnerabilities.
The results were striking. IVF-born offspring had lower
birth weights. They gained weight faster than naturally conceived controls. By
adulthood, more than 80% were clinically obese, compared to significantly lower
rates in the control group. Their fasting glucose levels were elevated, and
glucose tolerance tests, the standard diagnostic screen for diabetes risk,
showed meaningful impairment.
These are not exotic laboratory findings. They mirror the
associations that epidemiologists have reported in human populations for years:
IVF-conceived children appear to carry modestly elevated risks for low birth
weight, cardiovascular markers, and metabolic dysfunction. The mechanisms
behind those associations have never been clearly established. This study
offers the most mechanistically coherent explanation yet proposed: the same
epigenetic disruption that impairs implantation also programs long-term metabolic
vulnerability into the embryo's developmental trajectory.
A Potential Fix Already Tested in Human Embryos
The most immediately significant finding of the paper may
be what happened when the researchers attempted to correct the problem.
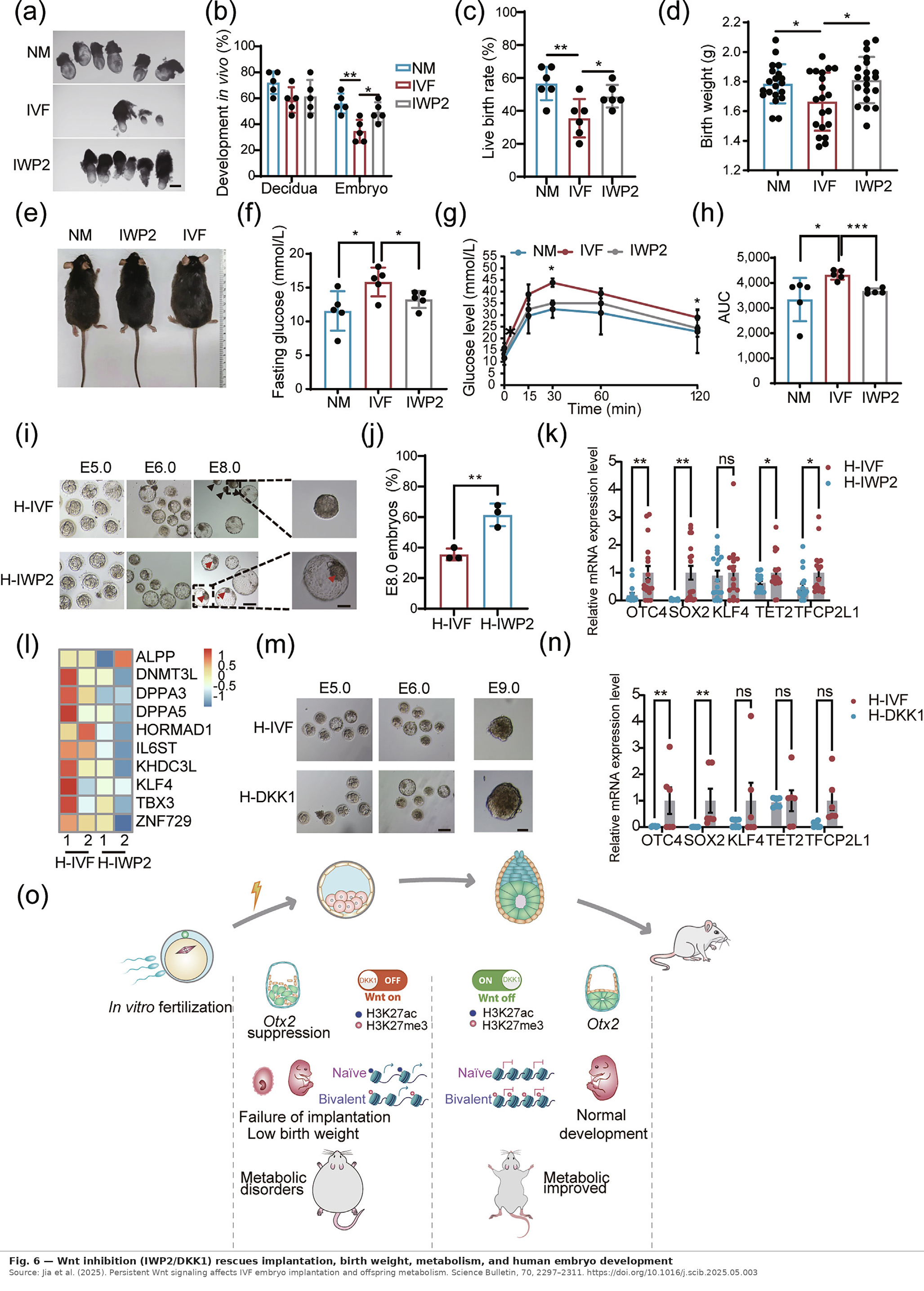
They treated IVF embryos with a Wnt-inhibiting compound
called IWP2 for just six hours at the late blastocyst stage, equivalent to Day
5 of human embryo culture, which is standard in most IVF laboratories. This
brief exposure was enough to partially restore the epigenetic landscape,
reactivate Otx2, and allow the naïve-to-primed transition to proceed normally.
The downstream effects were remarkable. Implantation rates
improved significantly. Live birth rates rose. Birth weights normalized. And
the metabolic abnormalities seen in IVF offspring, such as obesity and glucose
intolerance, were substantially ameliorated. A single six-hour chemical
intervention at the embryo culture stage appeared to rewrite the developmental
story all the way into adulthood.
The researchers then moved to human embryos, using 57
donated cleavage-stage embryos from IVF patients. Embryos treated with the Wnt
inhibitor at Day 5 showed measurably improved development by Day 8, a timepoint
when untreated control embryos had already begun degenerating. The naïve
pluripotency genes that should be switching off in preparation for implantation
were successfully downregulated in the treated embryos. A parallel experiment
using supplemental DKK1 protein, the natural Wnt brake that IVF embryos cannot
produce in sufficient quantities, produced similar improvements.
What This Means for the Future of IVF
The findings are preliminary, and the researchers are
careful to say so. IWP2 is a laboratory compound, not a clinical drug. The
human embryo experiments measured developmental progress in culture, not actual
pregnancy rates after transfer. Optimal dosing and timing have not yet been
established for human use. And the long-term safety of Wnt modulation in human
embryos remains entirely untested.
But the study does several important things. It identifies
a specific, measurable molecular defect that distinguishes IVF embryos from
naturally conceived ones. It provides a mechanistic explanation for both
implantation failure and offspring health risks, linking them to the same root
cause. And it demonstrates, in two species, that correcting that defect through
a brief pharmacological intervention at an already standard timepoint in the
IVF protocol produces measurable benefit.



