The silence of an intensive care unit is
deceptive, masking a high-stakes race where every second costs more than money.
For a patient sinking into the depths of sepsis, the enemy is often an
invisible "superbug" that has evolved to ignore the very antibiotics
designed to destroy it. This quest for speed is not new. Over a century ago,
researchers like Bronfenbrenner and Schlesinger (1918) were already
experimenting with rapid methods to identify bacteria, recognizing even then
that time is the most precious commodity in clinical microbiology. Yet, as
modern medicine faces the relentless dissemination of antimicrobial resistance,
the stakes have shifted from simple identification to decoding a pathogen's
entire genetic arsenal in real-time.
While traditional diagnostics require days to
grow bacteria in a laboratory, metagenomic next-generation sequencing offers a
culture-independent shortcut. The technical hurdle, however, remains immense.
In a typical clinical sample, the microbial signal is often buried under an
avalanche of human host DNA. To address this, specialized extraction methods
like the MolYsis basic kit are deployed to deplete host material, ensuring that
the final data is rich in microbial information. Even with clean data, the computational
burden of reconstructing these genomes can be crushing, often requiring
high-performance supercomputers. It is within this digital bottleneck that a
team led by Chang Liu (2024) introduced MetaGeneMiner, a tool designed to find
the needles in the genetic haystack using nothing more than a standard personal
computer.
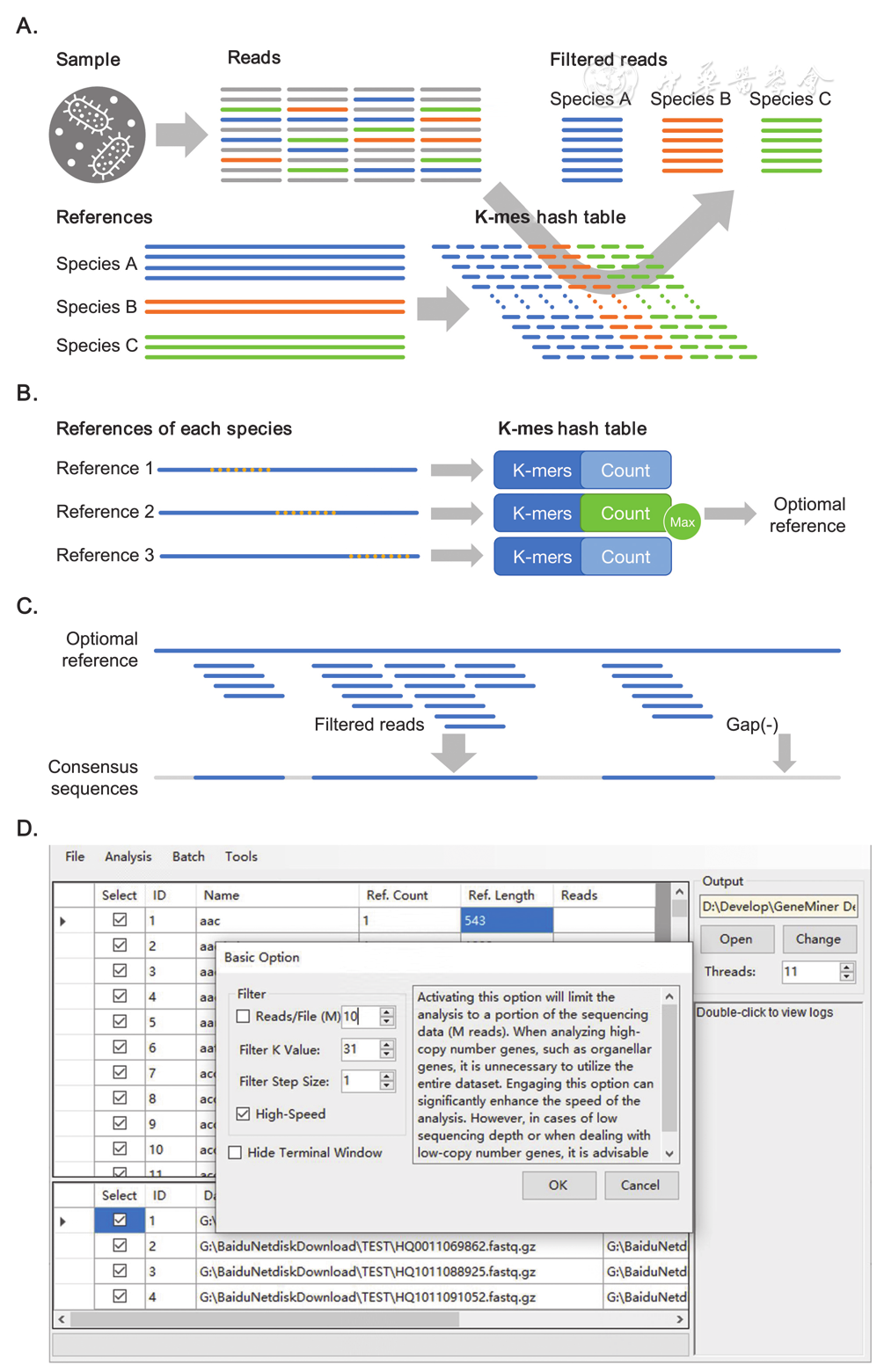
The algorithmic DNA of this new tool actually
evolved from a predecessor called GeneMiner2, which was originally built by Xie
et al. (2024) to recover target genes from low-coverage plant and animal
datasets. While the earlier software was a tool for evolutionary biologists,
MetaGeneMiner was specifically re-engineered for the chaos of clinical
diagnostics. By using a mathematical shortcut known as k-mer hashing, the
software can scan raw genetic reads and partition them toward specific targets
without the need for full, resource-intensive assembly. This approach mirrors
other recent breakthroughs in the field, such as the host-microbe models
developed by Kalantar et al. (2022), which achieved nearly perfect accuracy in
sepsis diagnosis by combining pathogen detection with the patient’s own immune
response.
During validation in the intensive care unit,
MetaGeneMiner successfully retrieved the coding sequences of dangerous
pathogens like Acinetobacter baumannii and Herpes Simplex Virus Type 1
from eight critically ill patients. The efficiency was striking where
conventional mapping methods might take seven hours, this targeted approach
finished in under two. For those infected with A. baumannii, a pathogen
known for its extreme genetic plasticity, the tool identified a diverse array
of resistance genes, including critical carbapenemases. This level of detail is
vital because, as Young et al. (2021) discovered in a massive study of Staphylococcus
aureus, the presence of specific resistance determinants is strongly
associated with a bacterium’s ability to survive in healthcare environments and
cause invasive disease.
Beyond the hospital bedside, this technology has
the potential to transform public health surveillance. Environmental studies,
such as those conducted in Marseille, France, have shown that municipal
wastewater serves as a mirror for the resistance genes circulating in a
population. By using targeted extraction tools, researchers can monitor these
wastewater landscapes for rare or emerging threats like colistin resistance
genes in minutes rather than weeks. This democratization of genomic analysis
means that a local clinic or environmental station can now perform the kind of
advanced tracking once reserved for elite research universities.
Scientific progress, however, rarely comes
without tension. A central debate in the community is whether the mere presence
of a resistance gene, as detected by software, truly guarantees that an
antibiotic will fail in a living patient. As the researchers themselves note,
biology is not always a binary switch; confirmation of resistance still
requires a careful look at a patient’s actual symptoms and other auxiliary
tests. Furthermore, tools like MetaGeneMiner are dependent on reference
databases, meaning they might struggle to flag entirely new, uncatalogued forms
of resistance.
CHALLENGES AND LIMITATIONS
Even the most sharp-eyed digital scout has its
blind spots. While MetaGeneMiner offers a revolutionary leap in speed for
identifying hospital-acquired infections, its architecture introduces a
specific set of constraints that remind us that software is a supplement to,
rather than a replacement for, clinical judgment. The tool’s greatest strength
its ability to ignore the noise of host DNA and focus on specific targets is
also its primary vulnerability. Unlike more computationally expensive methods
that explore a sample without preconceived notions, this software is a
specialist that requires a prerequisite map (Liu, 2024). To function, it must
be provided with reference sequences for the target taxa of interest, meaning
it effectively lacks the ability to discover entirely novel pathogens or
uncatalogued organisms that have yet to be recorded in a genetic database (Liu,
2024).
The technical elegance of the tool also involves
a delicate mathematical balancing act centred on the size of the genetic
fragments, or k-mers, it analyzes. This choice is a trade-off between
sensitivity and specificity. If a researcher sets the k-mer size too low, the
software risks becoming bogged down by non-specific background data, which
slows the analysis and can lead to less accurate sequences (Liu, 2024).
Conversely, a setting that is too high might cause the software to miss
divergent reads, resulting in a fragmented or incomplete assembly of the target
gene (Liu, 2024). Furthermore, this k-mer-based approach, while incredibly
fast, struggles with the complex terrain of highly repetitive or low-complexity
genetic sequences (Liu, 2024). In these regions, it cannot provide the same
level of detailed mapping for structural changes such as insertions, deletions,
or rearrangements that traditional alignment-based methods offer (Liu, 2024).
There is also the persistent, high-stakes
tension between the genetic blueprint and the physical reality of an infection.
Science has long known that the presence of a resistance gene does not always
guarantee that an antibiotic will fail when it meets the patient (Liu, 2024). A
bacterium might possess the weapon of resistance, but that weapon may remain
unexpressed or dormant due to various biological factors. Consequently, the
researchers are careful to state that "the presence of corresponding resistance
genes in microbes does not necessarily translate to a resistant phenotype"
(Liu, 2024). This gap means that for a doctor at the bedside, the software’s
output must always be weighed against the patient's actual symptoms and other
traditional diagnostic tests.
Finally, the scope of the tool’s validation
remains a work in progress. While it has demonstrated "proficient
performance" against pathogens such as Acinetobacter baumannii, it was designed
and optimized primarily for extracting pathogen genomes in a clinical setting
(Liu, 2024). The researchers admit that more work is needed before the tool can
be reliably moved into other complex arenas, such as studying the intricate
balance of the human gut microbiome or tracking the shifting biodiversity of
environmental samples (Liu, 2024). As we move toward a future of precision
medicine, these limitations suggest that our most powerful digital tools still
require a steady human hand to navigate the nuanced reality of human health.
Looking ahead, integrating these rapid genetic
scouts into routine care could fundamentally change the patient experience.
Instead of broad-spectrum "emergency" antibiotics that can
inadvertently drive further resistance, doctors may soon reach for targeted
therapies informed by the exact genetic blueprint of the infection. For the
patient in the intensive care unit, this shift from an educated guess to a
data-driven strike represents more than just a technological milestone. It is
the fulfillment of a century-long search for a truly rapid diagnosis, offering
a vital second chance when time is running out.




