Nepal Health News, IPAC & Research | The Health Thread
Top Stories
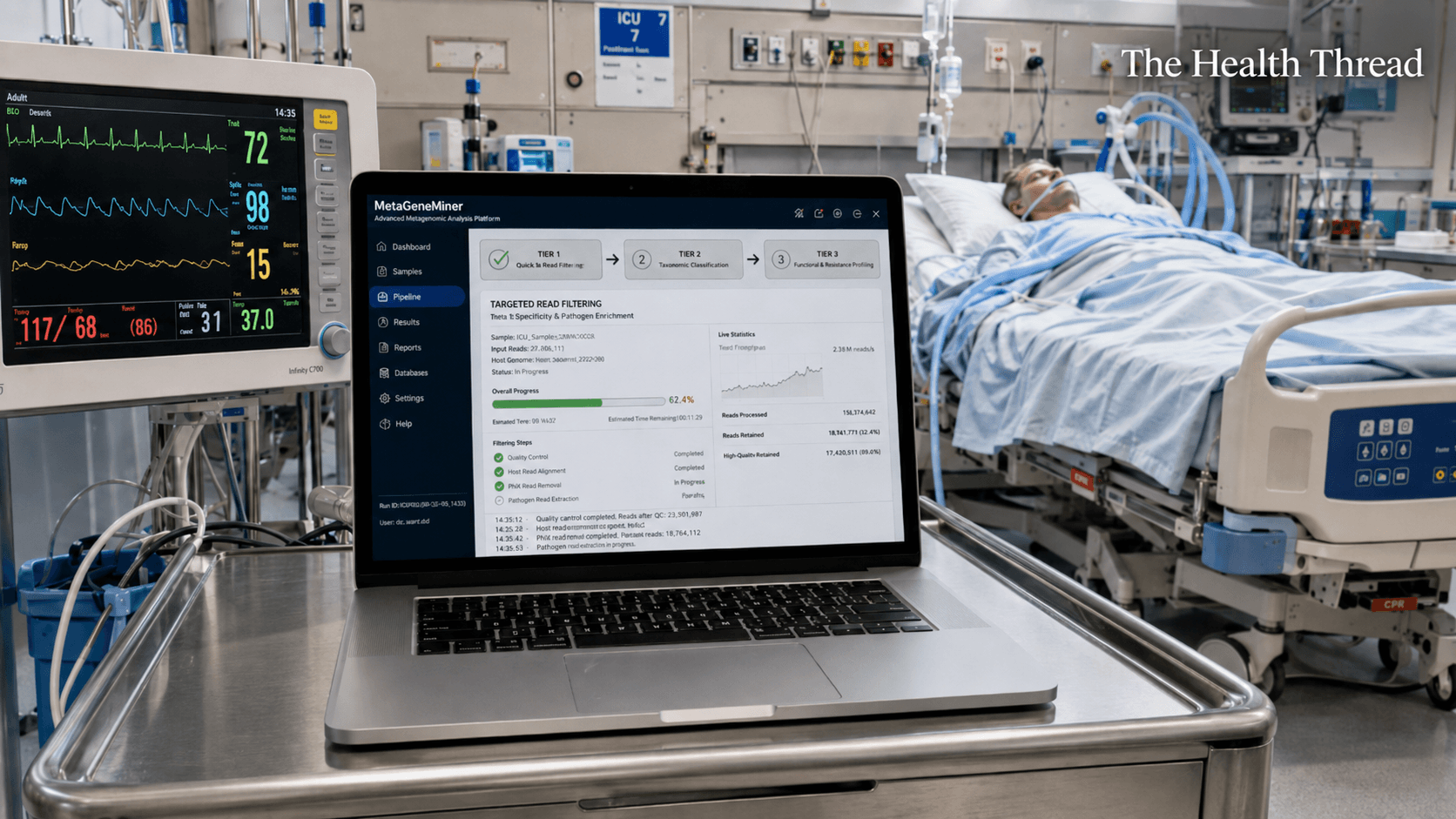
MetaGeneMiner and the High Stakes Search for Antibiotic Resistance
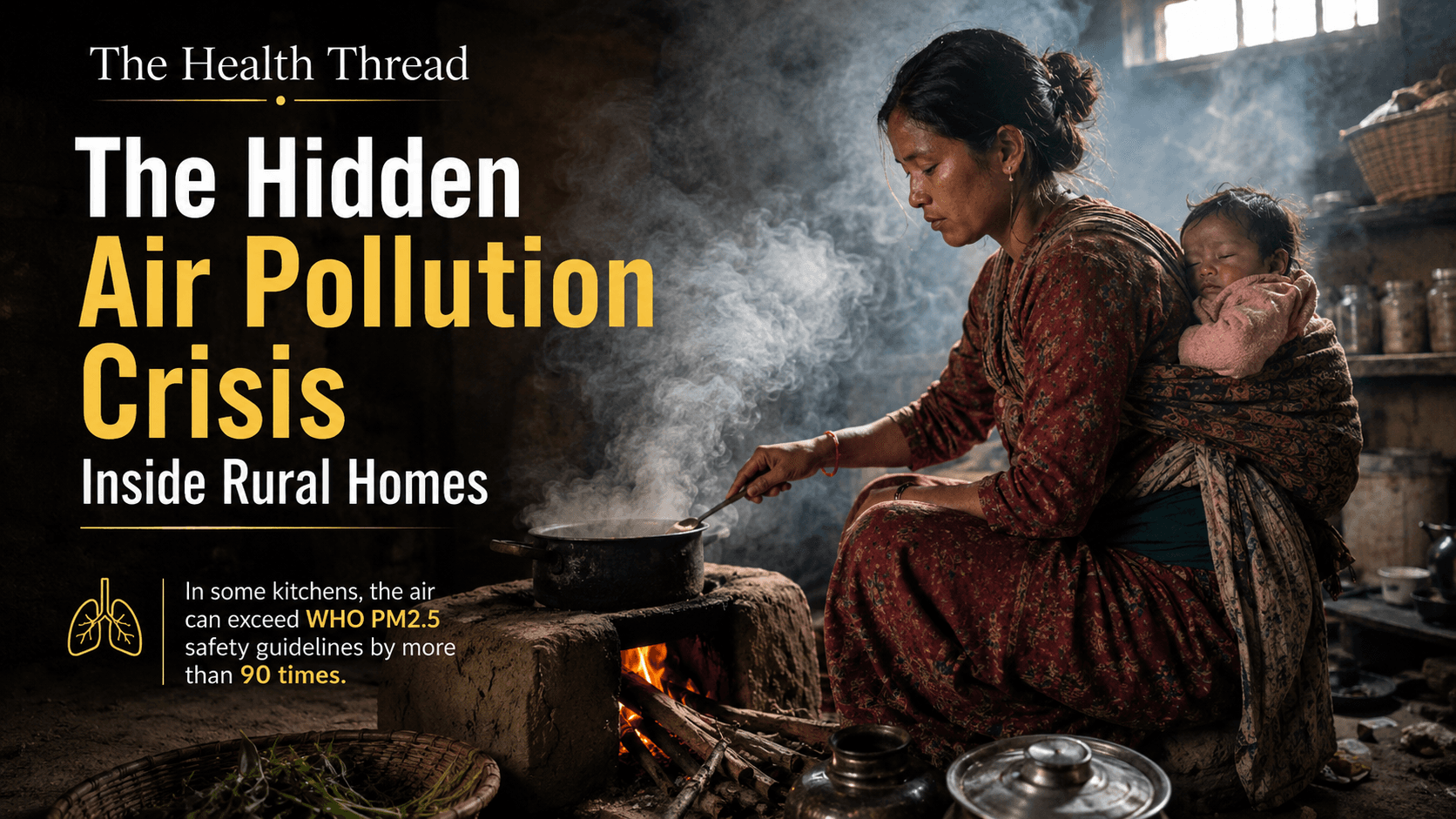
The Deadliest Room in the House: Indoor Air Pollution and South Asia's Most Overlooked Public Health Emergency
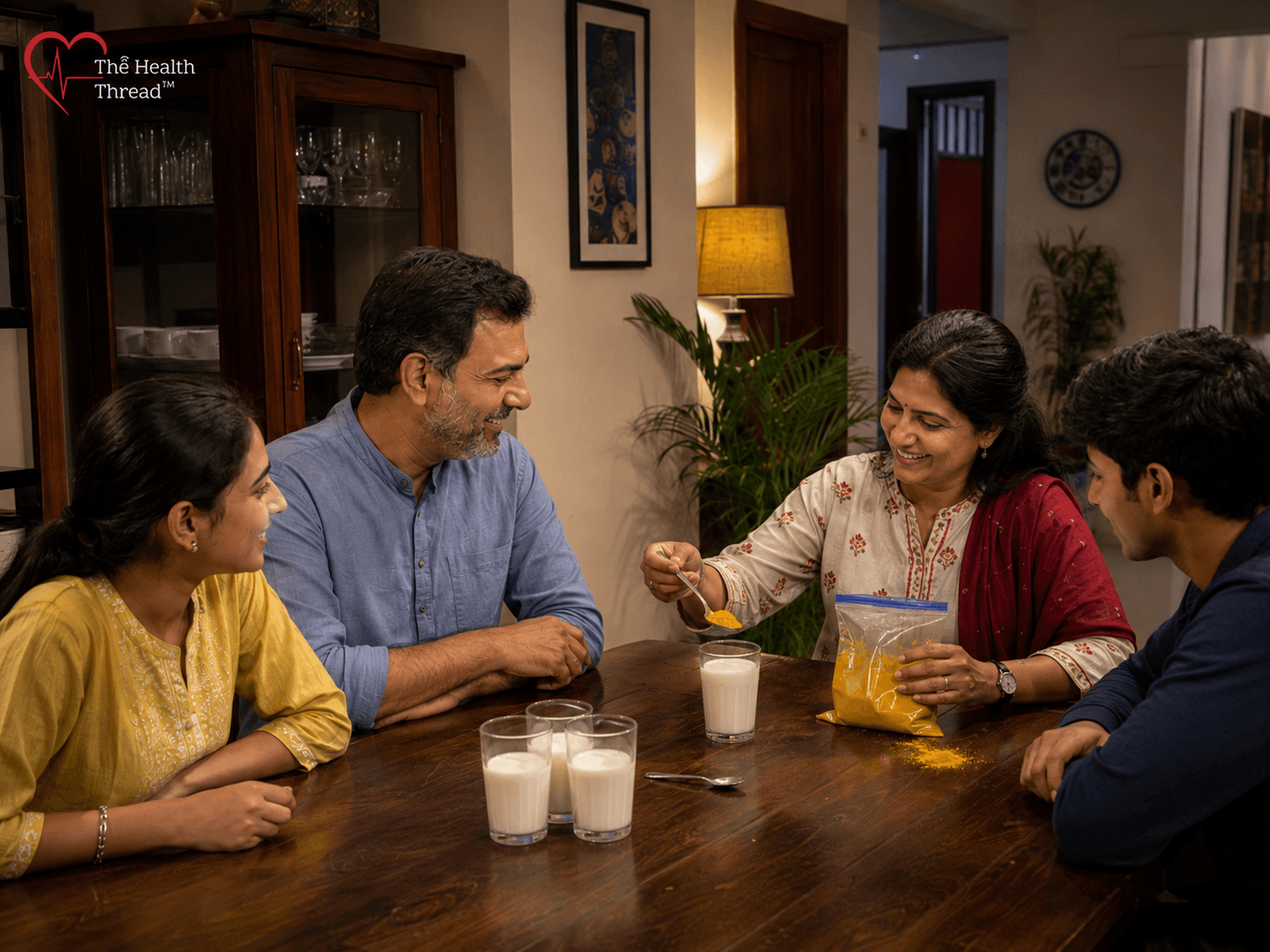
The Golden Milk Problem: What Turmeric Can and Cannot Do for You
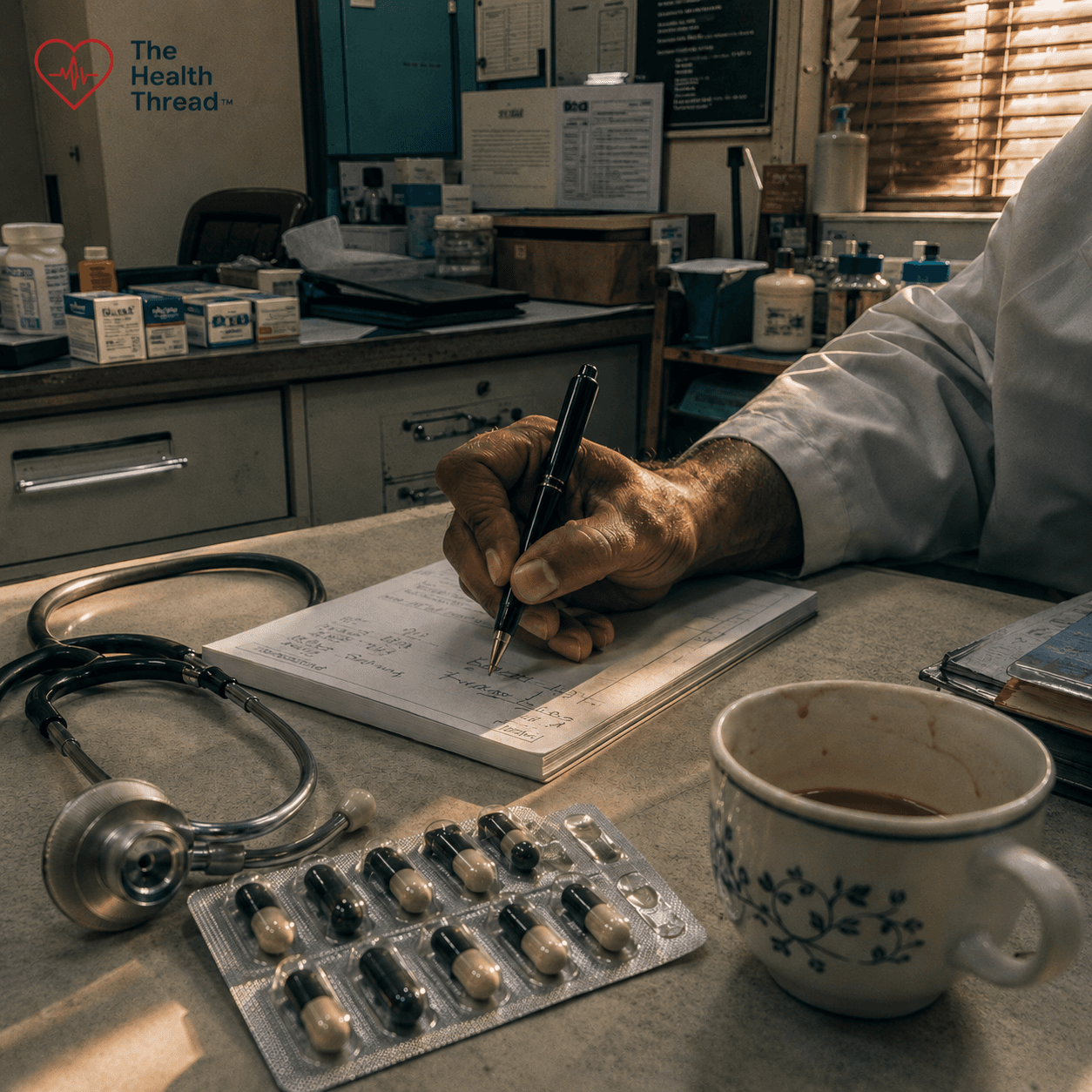
Prescribing Without Diagnosis: Antibiotic Overuse, Clinical Complicity, and the Coming Catastrophe of Antimicrobial Resistance
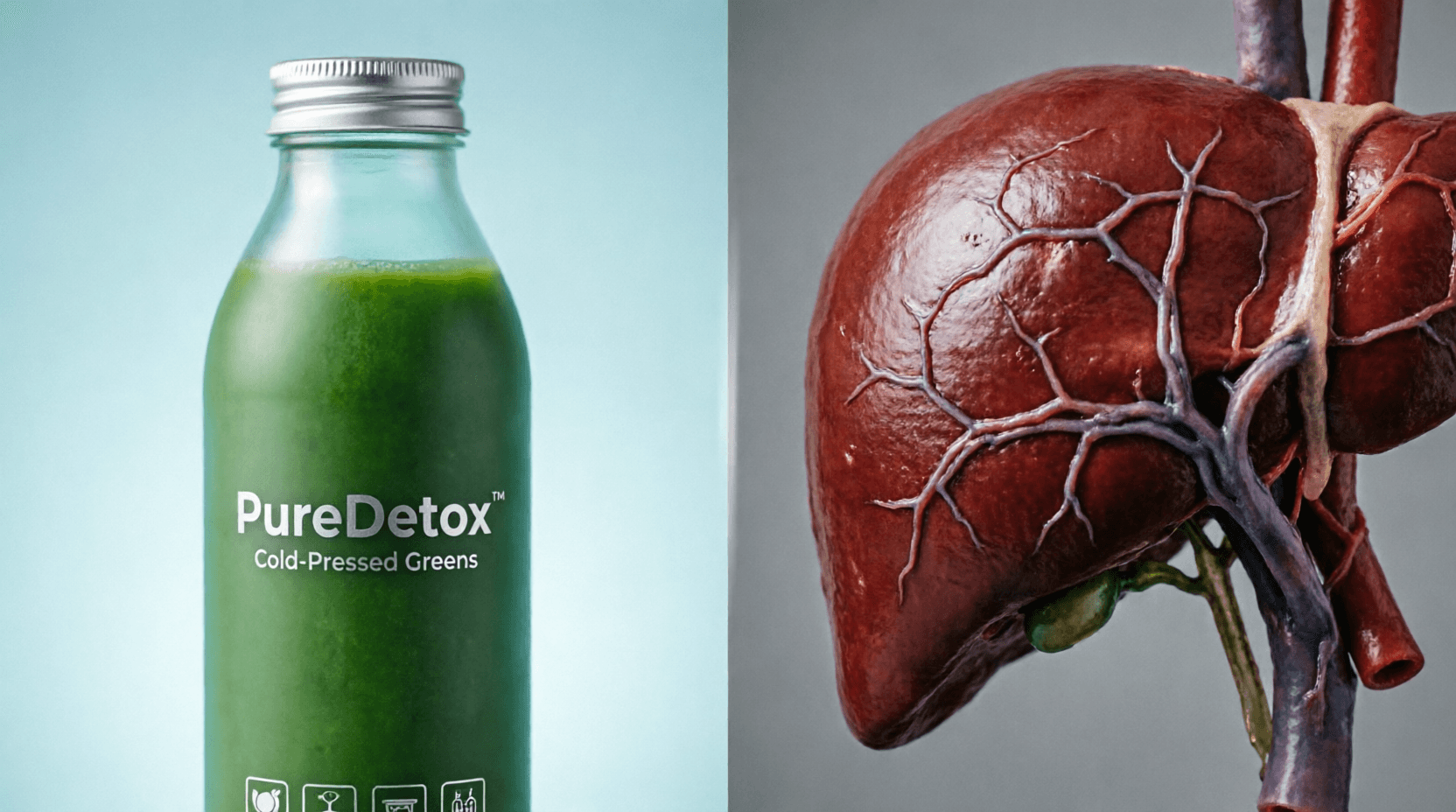
The Detox Industry and the Mythology of Liver Cleansing: A Scientific Examination
Your trusted source for Nepal health news, evidence-based IPAC guidelines, and the latest clinical research.
Research Watch
Latest Findings
More from Research Watch

Protecting the Smallest Lungs from the Hidden Grip of RSV in Kathmandu
Kamala Shrestha
The Heavy Burden of Bullying on Student Wellbeing in Nepal
Sabina Maharjan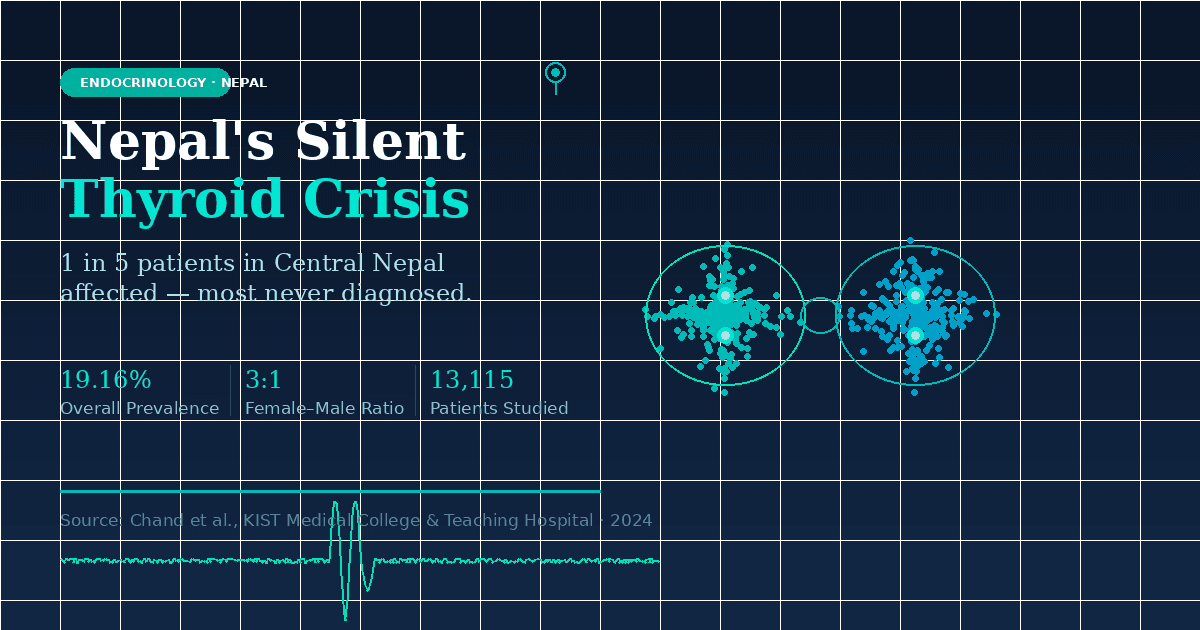
The Emerging Landscape of Thyroid Health in Central Nepal
Priya Lohani
How a Recent Western Nepal Study is Redefining Anemia Diagnosis
Anusha BastolaGlobal Health & Current Affairs
Full CoverageUnmasking the Crisis of Elder Abuse and Declining Health in Nepal
A recent study of 385 seniors in Kathmandu reveals that nearly one-third experience abuse, mostly psychological and financial, while chronic diseases like hypertension and diabetes go undertreated. Researchers are calling for urgent reform in elder care, legal protection, and geriatric health services across Nepal.
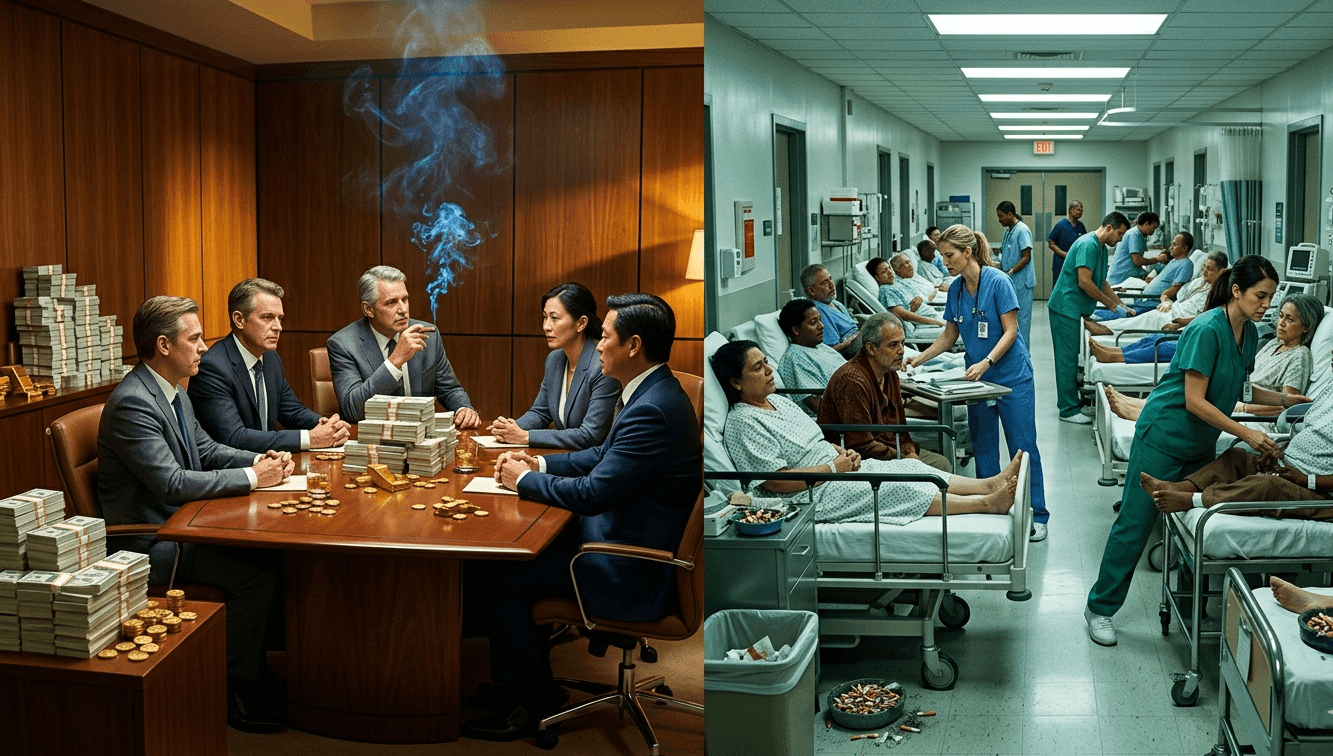
Will governments make the tobacco industry pay for all the harms it causes?
A global coalition is demanding that Big Tobacco be held financially accountable for $1.4 trillion in annual societal costs. The Make Big Tobacco Pay campaign urges governments to enforce WHO treaty obligations and ensure that the industry, not taxpayers, covers the full costs of its deadly and polluting products.
Nepal Boosts Child Health: New RUTF Procurement Targets Malnutrition
Nepal's Department of Health Services is progressing with the re-procurement of Ready-to-Use Therapeutic Food (RUTF). This essential nutrient-rich paste is crucial for treating severe acute malnutrition (SAM) in children, especially in remote areas. Ensuring a steady supply of RUTF is a vital step in safeguarding young lives and improving child health outcomes across the nation.
Read Update →Nepal's Health Watch: Gastrointestinal Illness Tops Recent Disease Reports, Prompting Public Awareness
Nepal's latest health bulletin reveals Acute Gastro Enteritis as the most reported condition, with 861 cases in a single week. This highlights the ongoing importance of public health surveillance and vigilance against common communicable diseases. Understanding symptoms, practicing good hygiene, and ensuring food and water safety are crucial preventive measures for the community.
Urgent Cheese Recall: Listeria Threat Prompts Clover Hill Dairy Action
WHO Unveils New Guidelines to Revolutionize Filovirus Disease Care
Rapid Decentralized Testing Boosts Ebola Response in DR Congo Outbreak
Uganda's Strong Ebola Response Highlights Critical Need for Regional Unity

Editor's Picks

The South Asian Trap: Why Alcohol Hits Nepal Harder
A 2026 study at Nepalgunj Medical College reveals a silent epidemic of alcoholic liver disease (ALD) in Nepal, with a 14% mortality rate among 384 hospitalized patients. The research found that South Asians are genetically more susceptible to liver damage, developing ALD with less alcohol consumption than Western populations. While men in their 40s comprised 80% of cases, women faced higher death rates (17.7% vs. 13.1%). With over 77% of patients presenting with jaundice and hepatic encephalopathy causing 81% of deaths, researchers urge immediate public health interventions, including routine screening and early detection programs, to address this preventable crisis.

Unmasking the Crisis of Elder Abuse and Declining Health in Nepal
A recent study of 385 seniors in Kathmandu reveals that nearly one-third experience abuse, mostly psychological and financial, while chronic diseases like hypertension and diabetes go undertreated. Researchers are calling for urgent reform in elder care, legal protection, and geriatric health services across Nepal.
Will governments make the tobacco industry pay for all the harms it causes?
A global coalition is demanding that Big Tobacco be held financially accountable for $1.4 trillion in annual societal costs. The Make Big Tobacco Pay campaign urges governments to enforce WHO treaty obligations and ensure that the industry, not taxpayers, covers the full costs of its deadly and polluting products.
Experts Urge Indonesia to Ratify Global Tobacco Treaty and Enforce Industry Accountability
Indonesia remains one of only 8 countries yet to ratify the WHO tobacco treaty. Over 1,500 health experts are now demanding action to protect millions from a deadly, costly epidemic.
More Stories
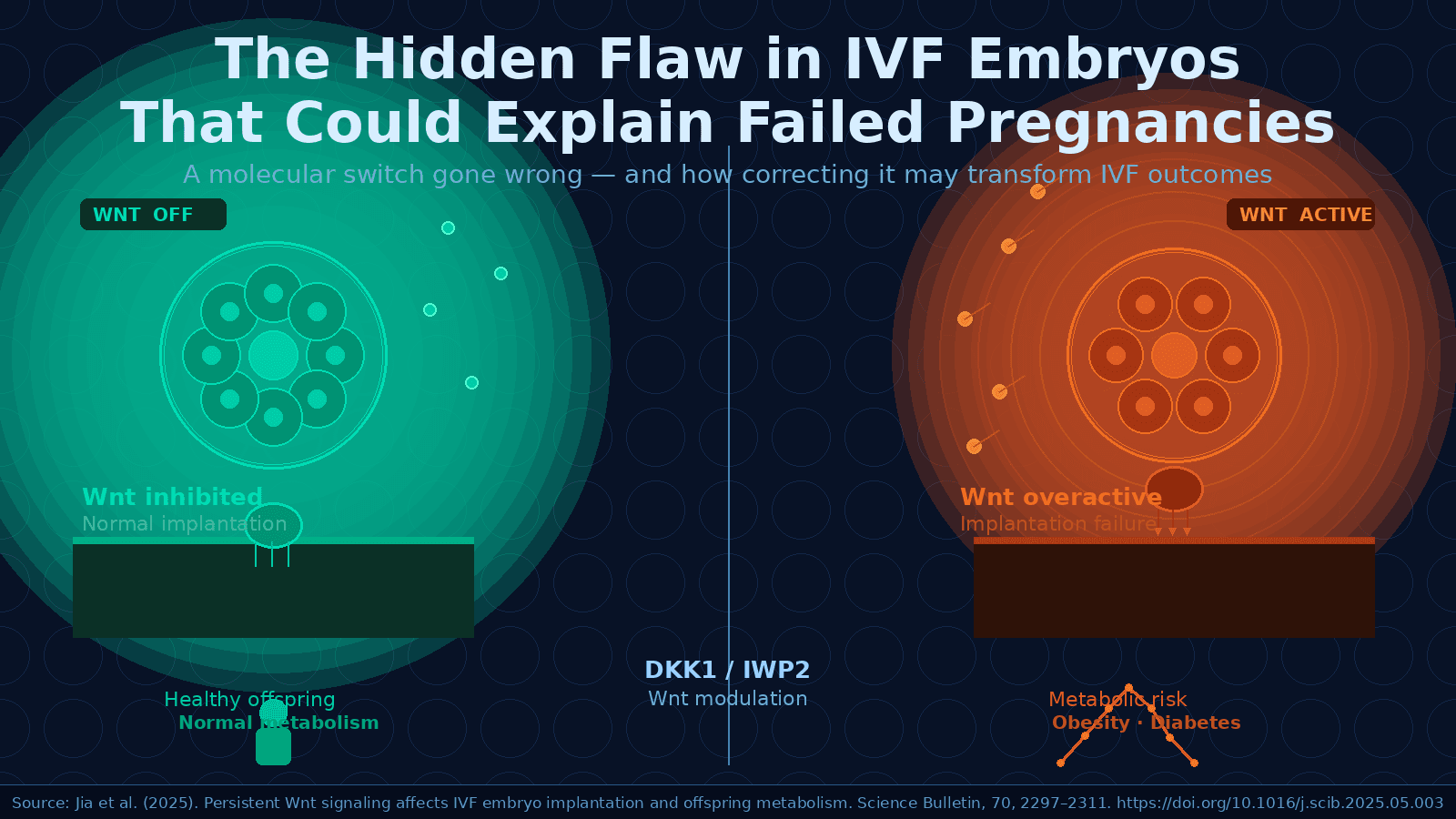
The Hidden Flaw in IVF Embryos That Could Explain Decades of Failed Pregnancies
A molecular flaw hidden inside IVF embryos present from the very first hours after fertilization may explain decades of unexplained implantation failures and health risks in IVF-conceived children. New research from Tongji University identifies a signalling pathway called Wnt that runs persistently out of control in IVF embryos, locking them in a developmental state that prevents successful implantation. Remarkably, a six-hour chemical intervention at the blastocyst stage was enough to correct the flaw, improve implantation rates, normalize birth weights, and protect offspring from obesity and diabetes in adulthood. The findings open a concrete path toward better embryo culture protocols and potentially, better outcomes for the millions of families who turn to IVF each year.
The invisible must get served first by a legally binding treaty for older persons
UN drafts a legally binding treaty to protect older persons' human rights. Ageism and discrimination end here. Older adults demand rights, not charity. Development justice for all ages.
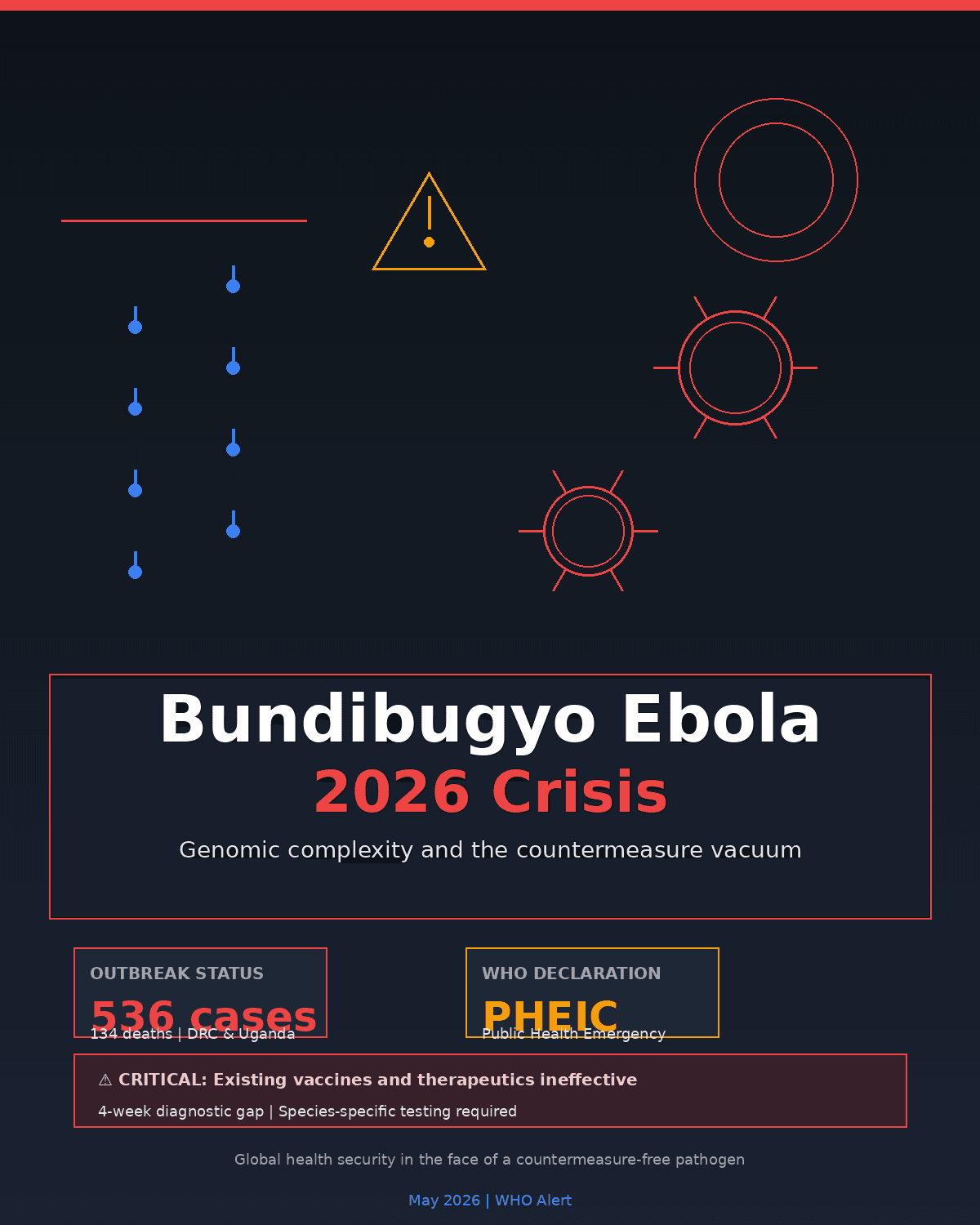
Beyond the Zaire Paradigm: Genomic Complexity and the 2026 Bundibugyo Ebola Crisis
WHO declares rare Bundibugyo Ebola outbreak a global health emergency. 536 suspected cases, 134 deaths in DRC/Uganda. Existing vaccines ineffective; the diagnostic gap delays detection by 4 weeks.

Feminist Lens on AMR: Why Gender Inequality Fuels Drug Resistance
Gender inequality fuels antimicrobial resistance (AMR). Women, girls, and gender‑diverse people face harmful norms, caregiving burdens, violence, stigma, and limited access to timely healthcare, all of which increase infection risk and inappropriate antibiotic use. AMR disproportionately affects those who cannot seek or complete treatment due to social, economic, and cultural barriers. A feminist, rights‑based, gender‑transformative AMR response is essential to ensure early diagnosis, equitable care, and policies that protect the most marginalized.

The Global Race for Hantavirus Immunity
A global push to develop the first licensed hantavirus vaccine has accelerated after the deadly 2026 Andes virus outbreak on the MV Hondius. Advances in structural biology, mRNA engineering, DNA platforms, and freezer‑free stabilization technologies are reshaping vaccine development. Despite scientific momentum, limited commercial incentives and biological challenges continue to delay progress. With climate change driving more frequent outbreaks, coordinated global efforts like CEPI’s 100 Days Mission aim to transform future hantavirus events from crises into manageable public‑health responses.
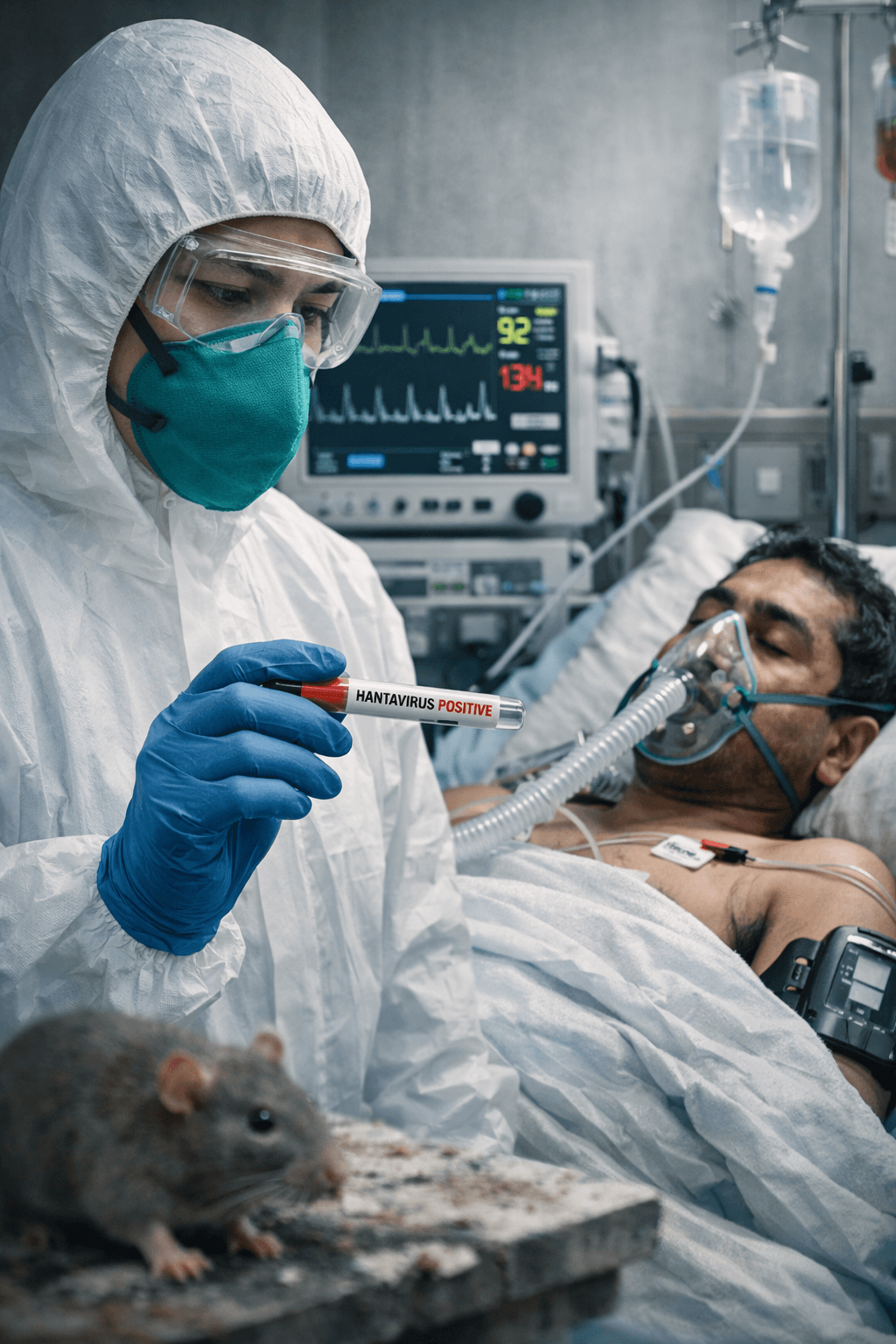
Understanding Hantavirus and Nepal’s Preparedness
A deadly Hantavirus outbreak on the MV Hondius cruise ship in May 2026 reignited global concern about this rodent‑borne virus, a threat that already affects Nepal. Hantaviruses, carried by rats, mice, and voles, spread when virus‑contaminated dust becomes airborne. In Asia, they cause Hemorrhagic Fever with Renal Syndrome (HFRS); in the Americas, the far deadlier Hantavirus Pulmonary Syndrome (HPS).
Health News
See all
संयोगले होइन, नियोजित रूपमा: विश्वव्यापी संक्रामक रोग वित्तीय सहयोगमा संरचनागत असमानता
The Deadliest Room in the House: Indoor Air Pollution and South Asia's Most Overlooked Public Health Emergency
Unmasking the Crisis of Elder Abuse and Declining Health in Nepal
Will governments make the tobacco industry pay for all the harms it causes?
Turning development justice analysis into collective actions
Mind, Body & Fitness
In Depth
Long Reads
Policy & Public Health
The Deadliest Room in the House: Indoor Air Pollution and South Asia's Most Overlooked Public Health Emergency
Experts Urge Indonesia to Ratify Global Tobacco Treaty and Enforce Industry Accountability
The invisible must get served first by a legally binding treaty for older persons
Feminist Lens on AMR: Why Gender Inequality Fuels Drug Resistance
Nepal’s Rapid Transition from Youth Bulge to Ageing Society
Specialized Care

Explore Health Topics
Get The Health Thread delivered to your inbox
Join thousands of readers who start their week with our curated health news, research breakthroughs, and expert analysis. Free, every Monday.
No spam, ever. Unsubscribe anytime.
“Ethical Health Journalism, from Kathmandu to the World”
The Health Thread bridges the gap between complex medical research and everyday readers.