Nepal Health News, IPAC & Research | The Health Thread

Top Stories
Hold the line: Fulfil the 2027 #EndTB commitments without shifting goalposts

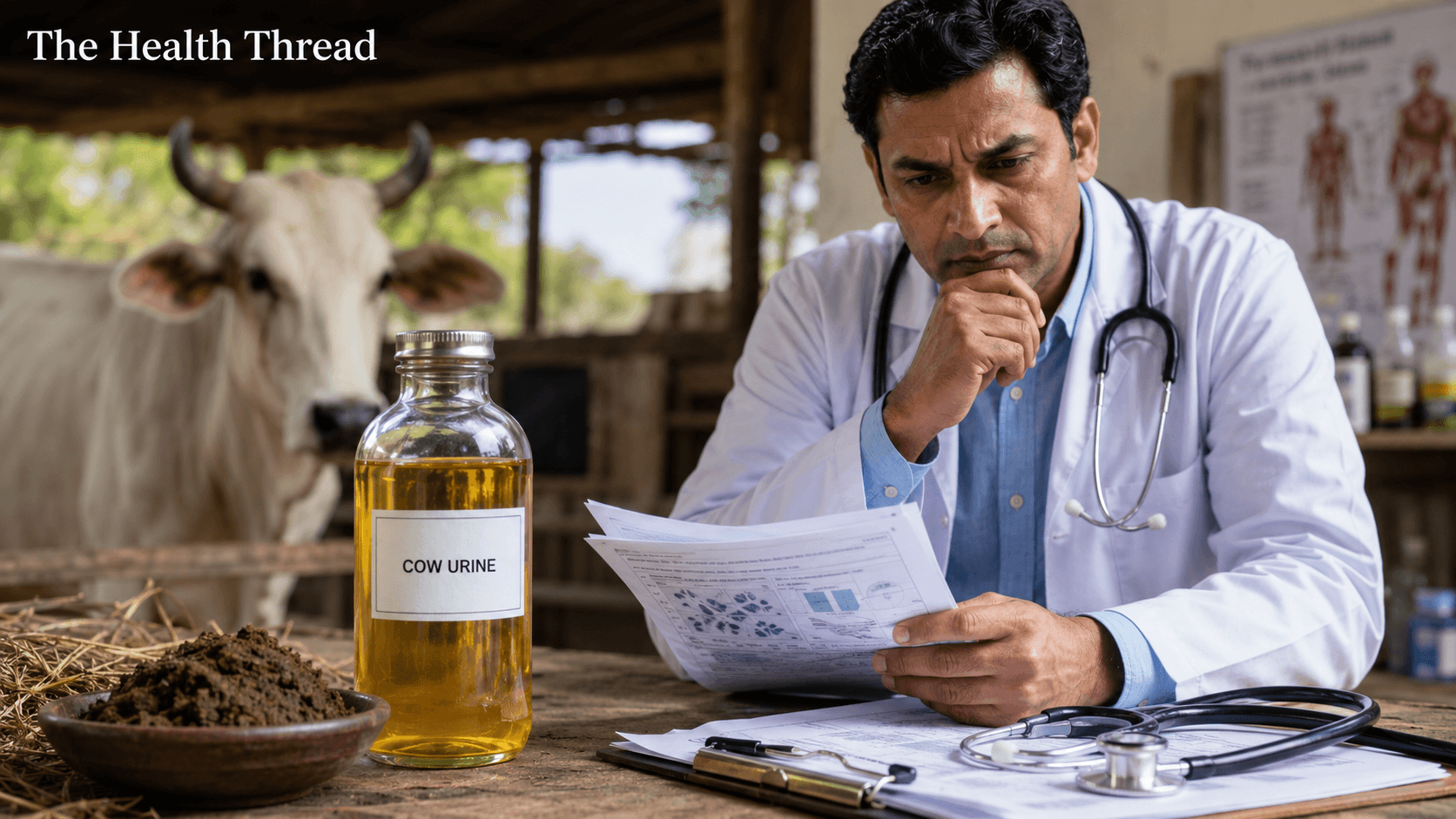
कुनै पनि पिसाब पवित्र हुँदैन: गाईको पिसाब र विज्ञानबीचको द्वन्द्व
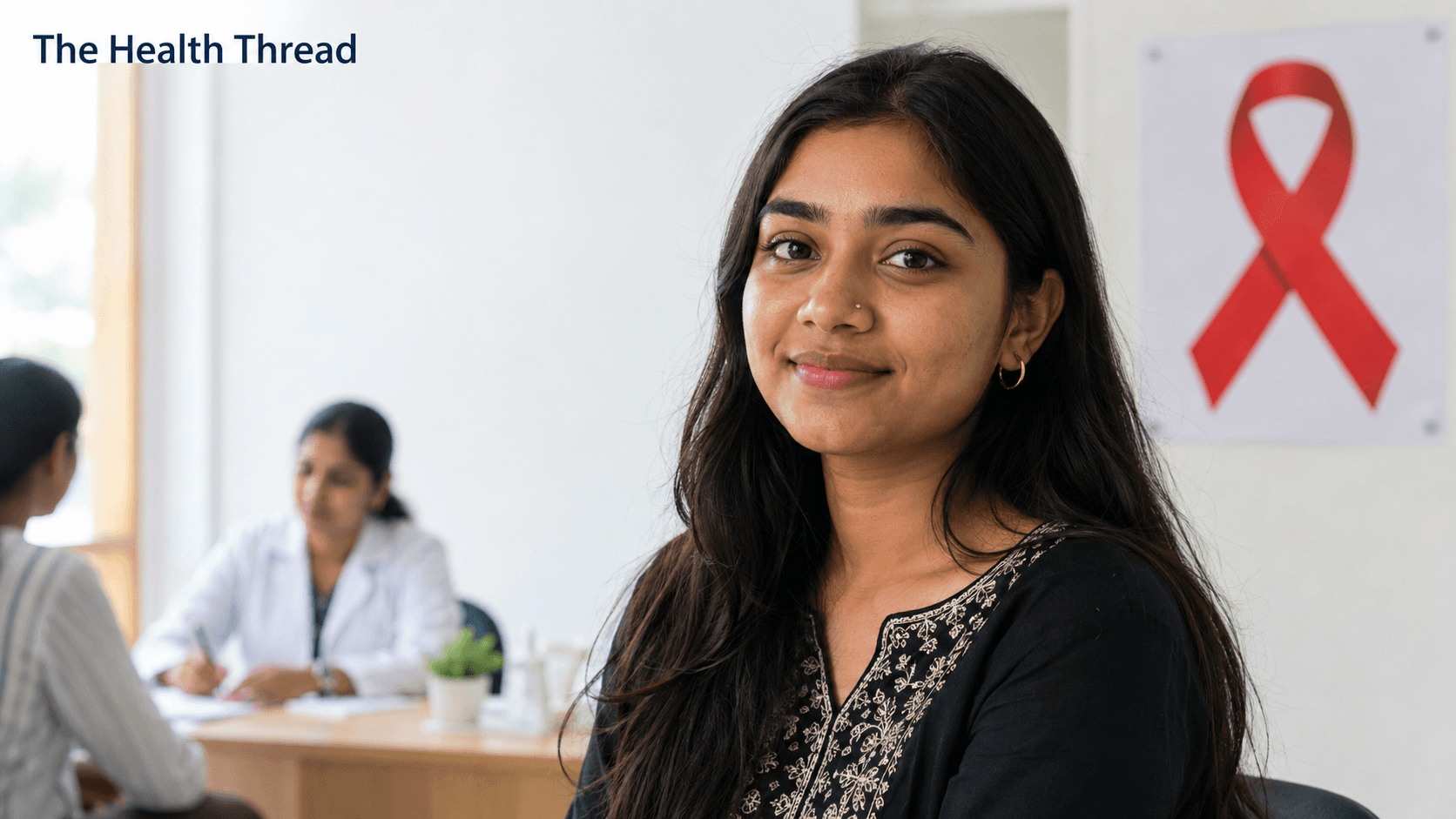
Rising above HIV diagnosis and turning pain into purpose
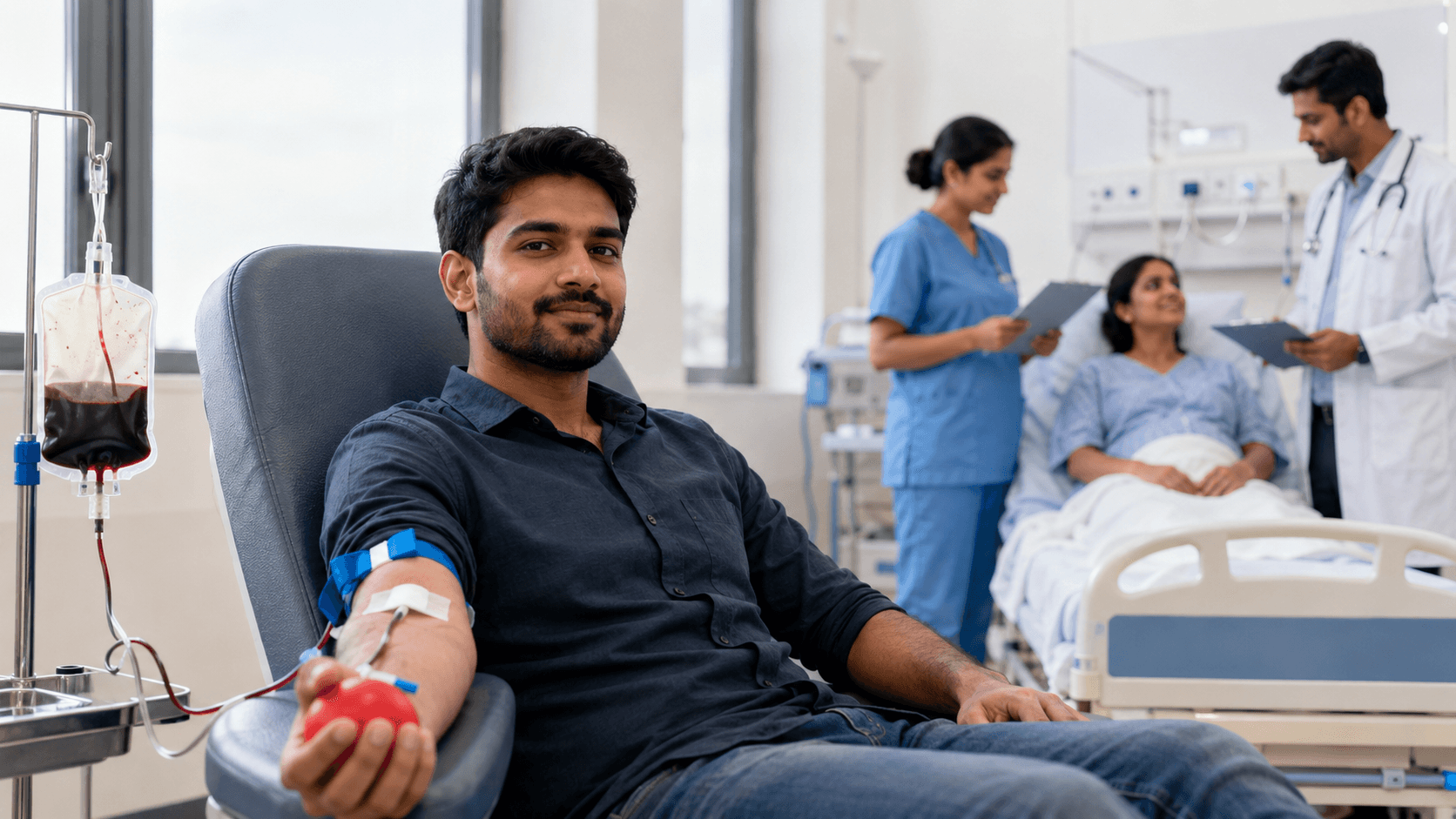
कहिल्यै कसैलाई कमजोर नबनाएको एक पिन्ट रगत: रक्तदानसम्बन्धी मिथ्या र त्यसको मूल्य चुकाइरहेका आमाहरू
बिहानको खाना नखाई हुँदैन भन्ने डर विज्ञानले होइन, नाफा खोज्ने कम्पनीहरूले चलाएको थियो।

Your trusted source for Nepal health news, evidence-based IPAC guidelines, and the latest clinical research.
Research Watch
Latest Findings
More from Research Watch

Frontline Perspectives on Nursing Leadership in Nepal
Liza Nagarkoti
Protecting the Smallest Lungs from the Hidden Grip of RSV in Kathmandu
Kamala Shrestha
The Heavy Burden of Bullying on Student Wellbeing in Nepal
Sabina Maharjan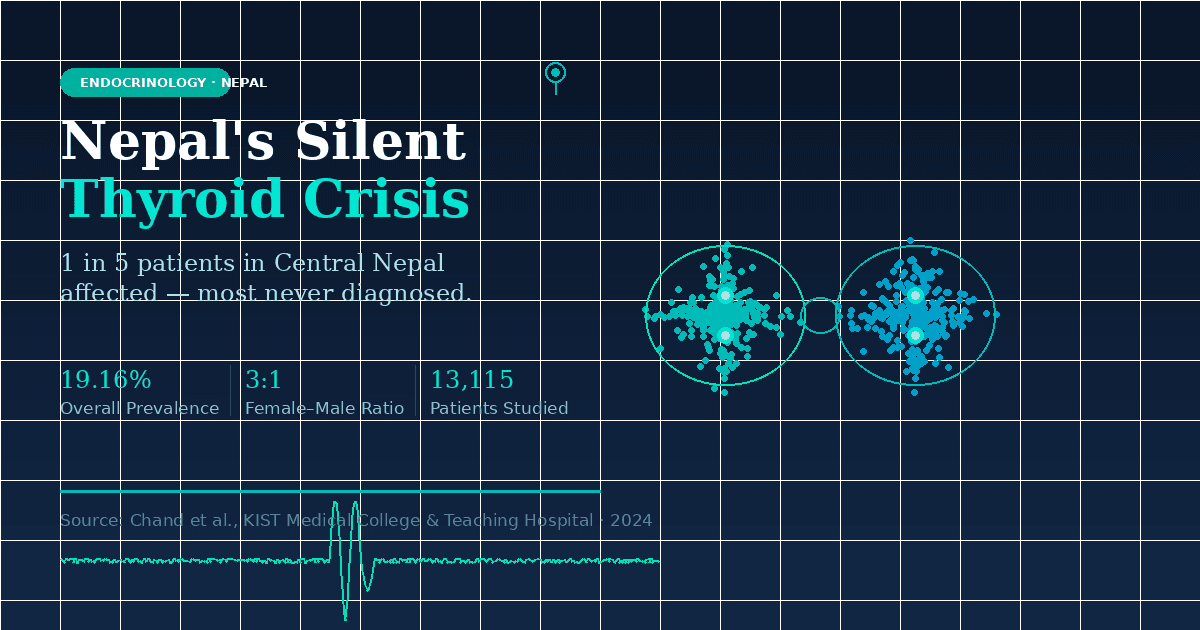
The Emerging Landscape of Thyroid Health in Central Nepal
Priya LohaniGlobal Health & Current Affairs
Full CoverageUnmasking the Crisis of Elder Abuse and Declining Health in Nepal
A recent study of 385 seniors in Kathmandu reveals that nearly one-third experience abuse, mostly psychological and financial, while chronic diseases like hypertension and diabetes go undertreated. Researchers are calling for urgent reform in elder care, legal protection, and geriatric health services across Nepal.
Will governments make the tobacco industry pay for all the harms it causes?
A global coalition is demanding that Big Tobacco be held financially accountable for $1.4 trillion in annual societal costs. The Make Big Tobacco Pay campaign urges governments to enforce WHO treaty obligations and ensure that the industry, not taxpayers, covers the full costs of its deadly and polluting products.
More Stories
All Global NewsYour Gut Health Matters: Insights from Nepal's Latest Disease Surveillance Report
Nepal's latest health surveillance for Week 28, 2026, reveals Acute Gastro Enteritis as the most reported condition, with 785 cases. This common 'stomach bug' underscores the ongoing importance of diligent hand hygiene, safe food practices, and clean drinking water to protect community health and prevent its widespread transmission.
Read Update →Nepal's Health Watch: Gastro Enteritis Cases Lead Latest Surveillance Report
Nepal's health authorities reported 732 cases of Acute Gastro Enteritis, making it the most frequently recorded condition in the latest surveillance bulletin for Week 29, 2026. This data, released by the Epidemiology and Disease Control Division, highlights the ongoing need for public awareness and preventive measures against common infectious diseases to safeguard community health.
Lidl US Expands Eridanous Shortbread Cookie Recall Over Undeclared Allergens
Ukrop's Recalls Spaghetti and Chicken Meals Over Foreign Object Concerns
South Sudan on High Alert for Bundibugyo Virus as Regional Outbreak Spreads
Cholera Crisis Deepens for Children in Sudan's El-Obeid Amidst Conflict
Editor's Picks
क्षयरोग सेवा दशकौँदेखि विस्तार भइरहँदा पनि हामी किन अझै क्षयरोग अन्त्य गर्ने बाटोमा छैनौँ?
क्षयरोगको उपचार र निदान सेवामा प्रगति भए पनि रोग अन्त्य गर्न यति मात्र पर्याप्त छैन। धुम्रपान, कुपोषण, मधुमेह, एचआईभी, गरिबी र कमजोर स्वास्थ्य पहुँचजस्ता मूल कारणलाई सम्बोधन नगरेसम्म नयाँ क्षयरोगका घटना घट्दैनन्। अब उपचारसँगै रोकथाम, समयमै स्क्रिनिङ, स्थानीय नेतृत्व र बहुक्षेत्रीय सहकार्यलाई क्षयरोग उन्मूलनको मुख्य आधार बनाउनुपर्छ।
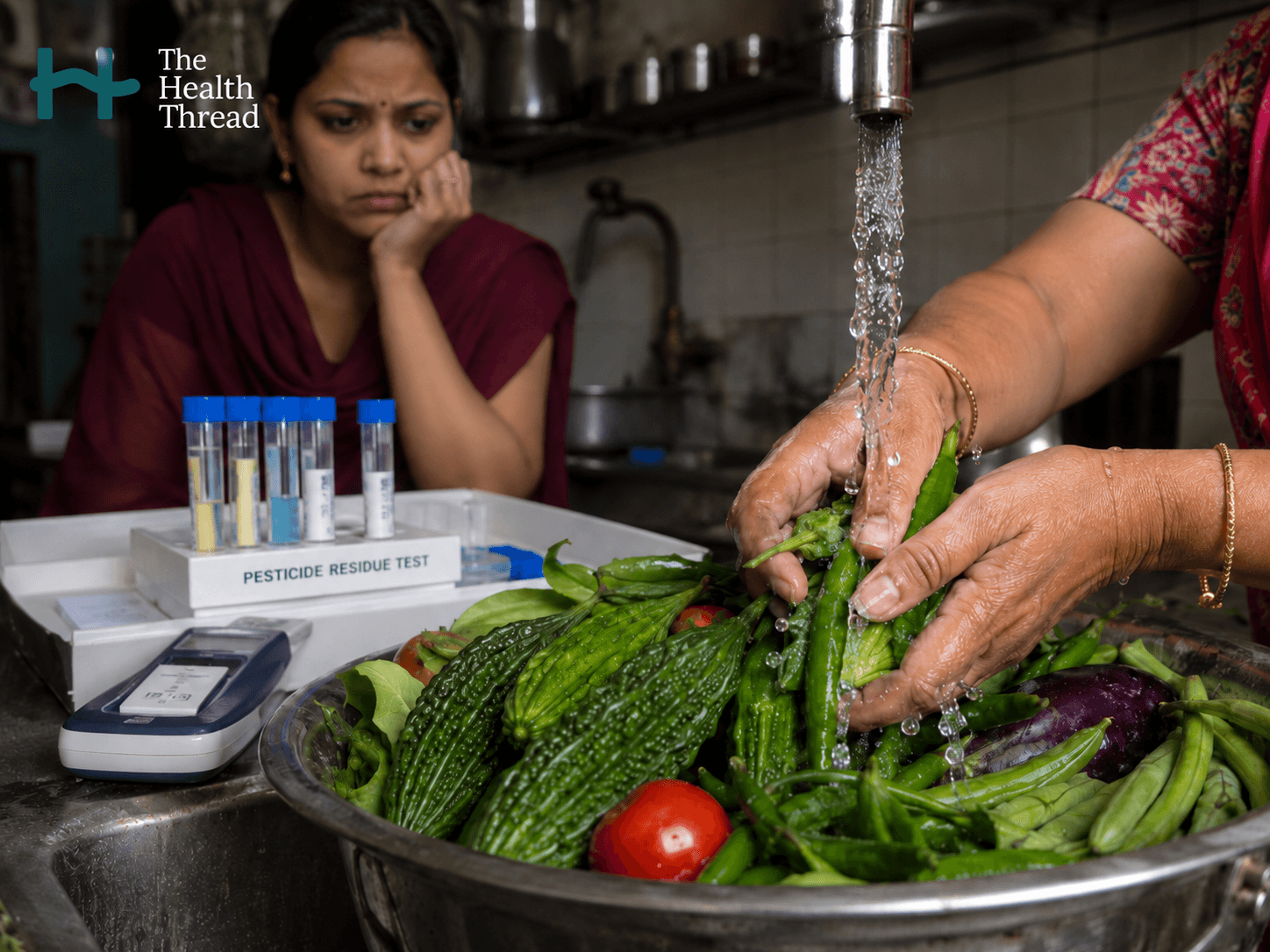
धोएर मात्रै सफा नहुने: दक्षिण एसियाको खानामा लुकेको विषादी संकट
तरकारी र चामलमा भेटिएका विषादी अवशेषले दक्षिण एसियाको खाद्य सुरक्षा संकटलाई गम्भीर बनाएको छ। सबै विषादी पानीले धुँदा हट्दैनन्, विशेषगरी बिरुवाभित्र सोसिएका सिस्टेमिक विषादी। कमजोर अनुगमन, विषादी छरेपछि कुर्नुपर्ने समय नपर्खी बजारमा पठाउने चलन र कडा कारबाहीको अभावले उपभोक्ताको थालसम्म जोखिम पुर्याइरहेको छ।
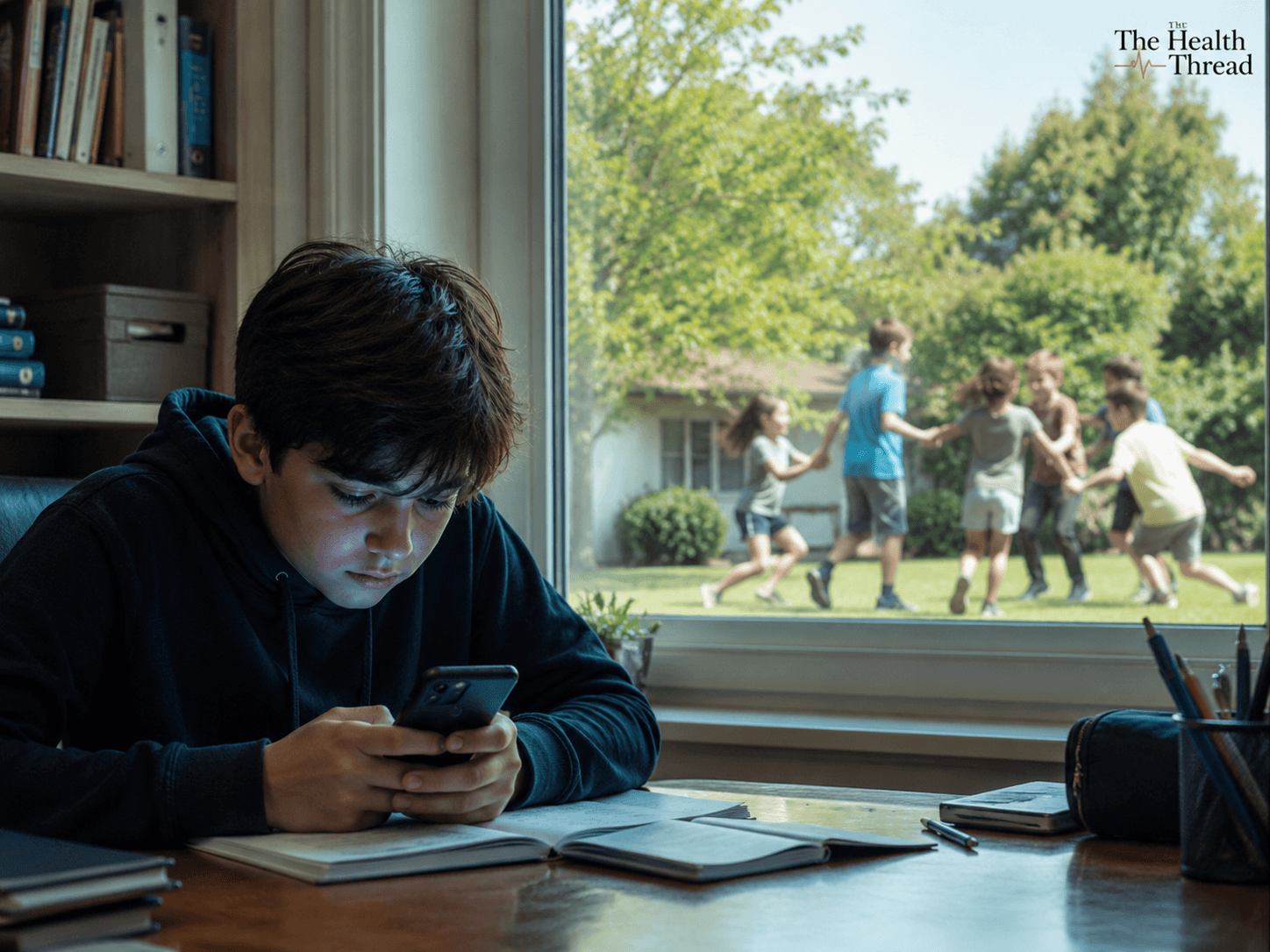
स्क्रिनले खोस्दै गएको बाल्यकाल: स्मार्टफोन, सामाजिक सञ्जाल र बालबालिकाको मानसिक स्वास्थ्य
स्मार्टफोन र सामाजिक सञ्जालले बालबालिकाको ध्यान, निद्रा, पढाइ, मानसिक स्वास्थ्य र सामाजिक सीपमा गहिरो असर पार्न थालेको प्रमाण बढ्दो छ। विश्वका धेरै देशले विद्यालयमा फोन प्रयोगमाथि कडा नीति बनाइसकेका छन्। अब नेपालले पनि बालबालिकाको भविष्य जोगाउन फोन मुक्त विद्यालय र जिम्मेवार डिजिटल प्रयोगबारे गम्भीर निर्णय लिनुपर्ने समय आएको छ।
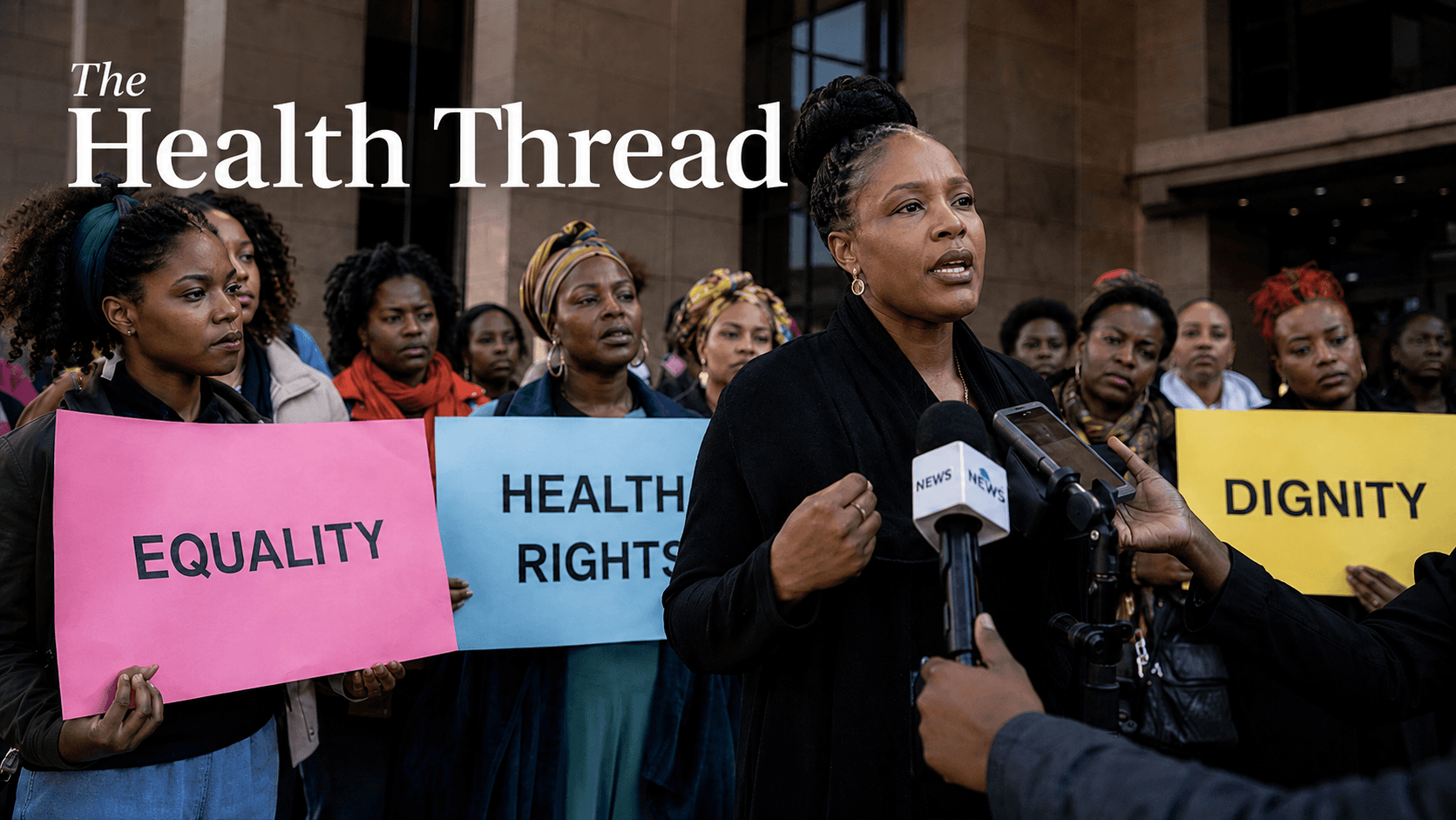
अफ्रिकामा लैङ्गिक समानता र स्वास्थ्य अधिकारविरुद्ध बढ्दो पितृसत्तात्मक प्रतिरोध
अफ्रिकामा प्रस्तावित नयाँ मस्यौदा बडापत्रले परिवार, संस्कृति र सार्वभौमिकताको नाममा लैङ्गिक समानता, स्वास्थ्यको अधिकार र मानव अधिकारका उपलब्धिहरू कमजोर बनाउने खतरा बढाएको छ। अधिकारकर्मीहरूका अनुसार, यो प्रयास अफ्रिकाको मात्र समस्या होइन। एउटा क्षेत्रमा अधिकार फिर्ता लिने अभ्यास संसारका अन्य ठाउँका लागि पनि खतरनाक उदाहरण बन्न सक्छ। उनीहरूले मापुटो प्रोटोकलको रक्षा गर्दै लैङ्गिक समानता, प्रजनन स्वास्थ्य अधिकार र मानव मर्यादालाई अटल मानव अधिकारका रूपमा अघि बढाउन विश्वव्यापी ऐक्यबद्धताको आह्वान गरेका छन्।
More Stories
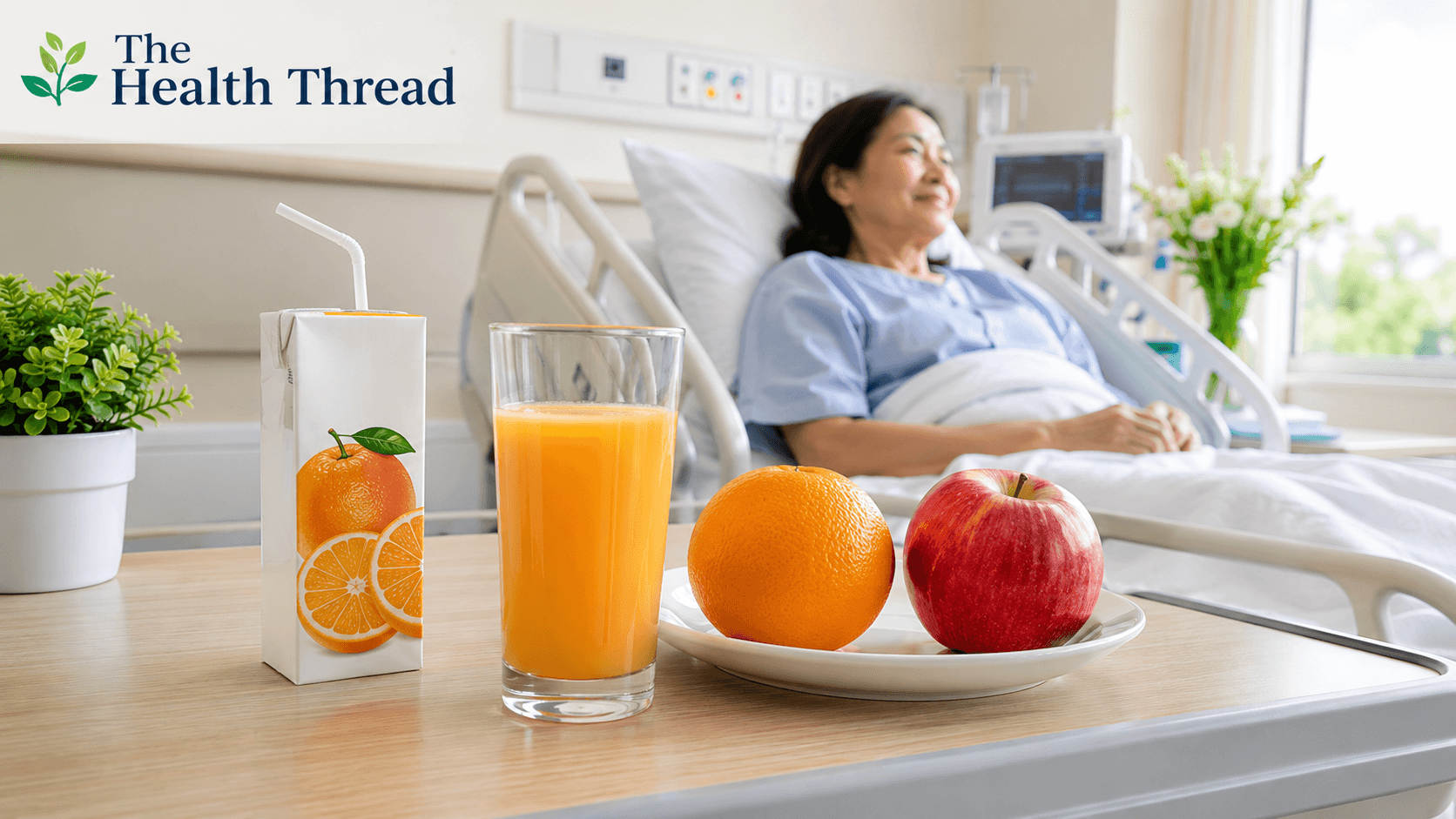
बिरामीलाई दिने जुस: पौष्टिक आहार कि फलको नाममा गुलियो भ्रम?
नेपालमा बिरामी भेट्न जाँदा जुस लैजाने चलन सामान्य छ। तर एक गिलास जुस र एउटा सिंगो फल एउटै होइनन्। जुस बनाउँदा फलको फाइबर र गुदीको ठूलो हिस्सा हट्छ, जसले रगतमा चिनी छिटो बढाउन सक्छ। अझ बजारमा “फलको जुस” भनेर बेचिने सबै उत्पादनहरू साँच्चिकै फलको जुस नहुन पनि सक्छन्। यो लेखले जुस, फाइबर, चिनी, मधुमेह जोखिम र दक्षिण एसियाली बजारमा जुसको नाममा बेचिने उत्पादनबारे वैज्ञानिक प्रमाणका आधारमा स्पष्ट रूपमा बुझाउँछ।
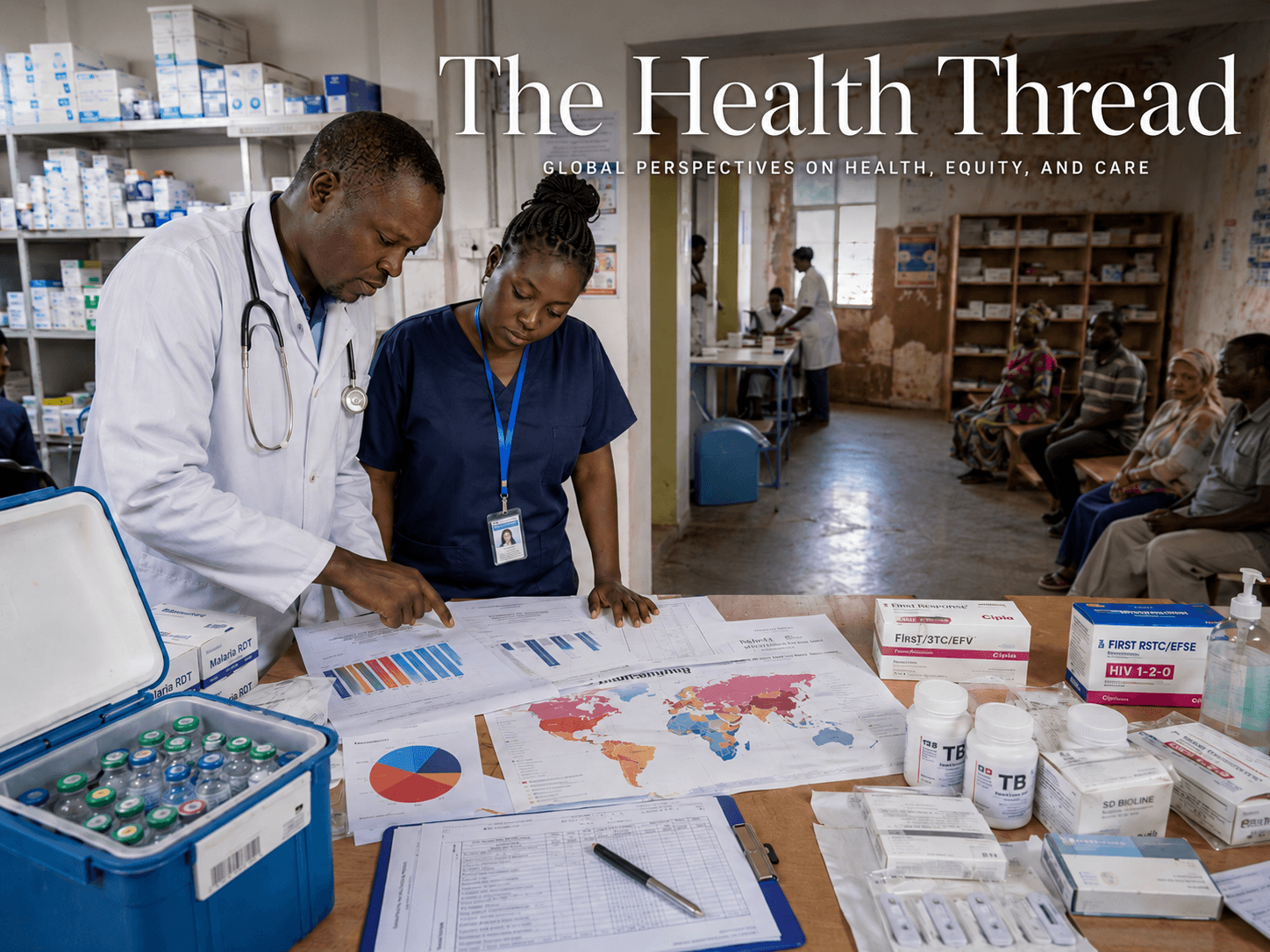
संयोगले होइन, नियोजित रूपमा: विश्वव्यापी संक्रामक रोग वित्तीय सहयोगमा संरचनागत असमानता
विश्वव्यापी संक्रामक रोगको संकट केवल रोगको समस्या होइन, यो असमान स्वास्थ्य प्रणालीको परिणाम हो। HIV, क्षयरोग, उपेक्षित उष्णकटिबन्धीय रोगहरू र महामारी तयारीमा देखिएको वित्तीय कटौतीले गरिब देशहरूलाई सबैभन्दा बढी जोखिममा पारेको छ। विज्ञान, औषधि र उपचार उपलब्ध भए पनि, राजनीतिक निर्णय र असमान लगानीका कारण लाखौँ रोक्न सकिने मृत्युहरू अझै जारी छन्।
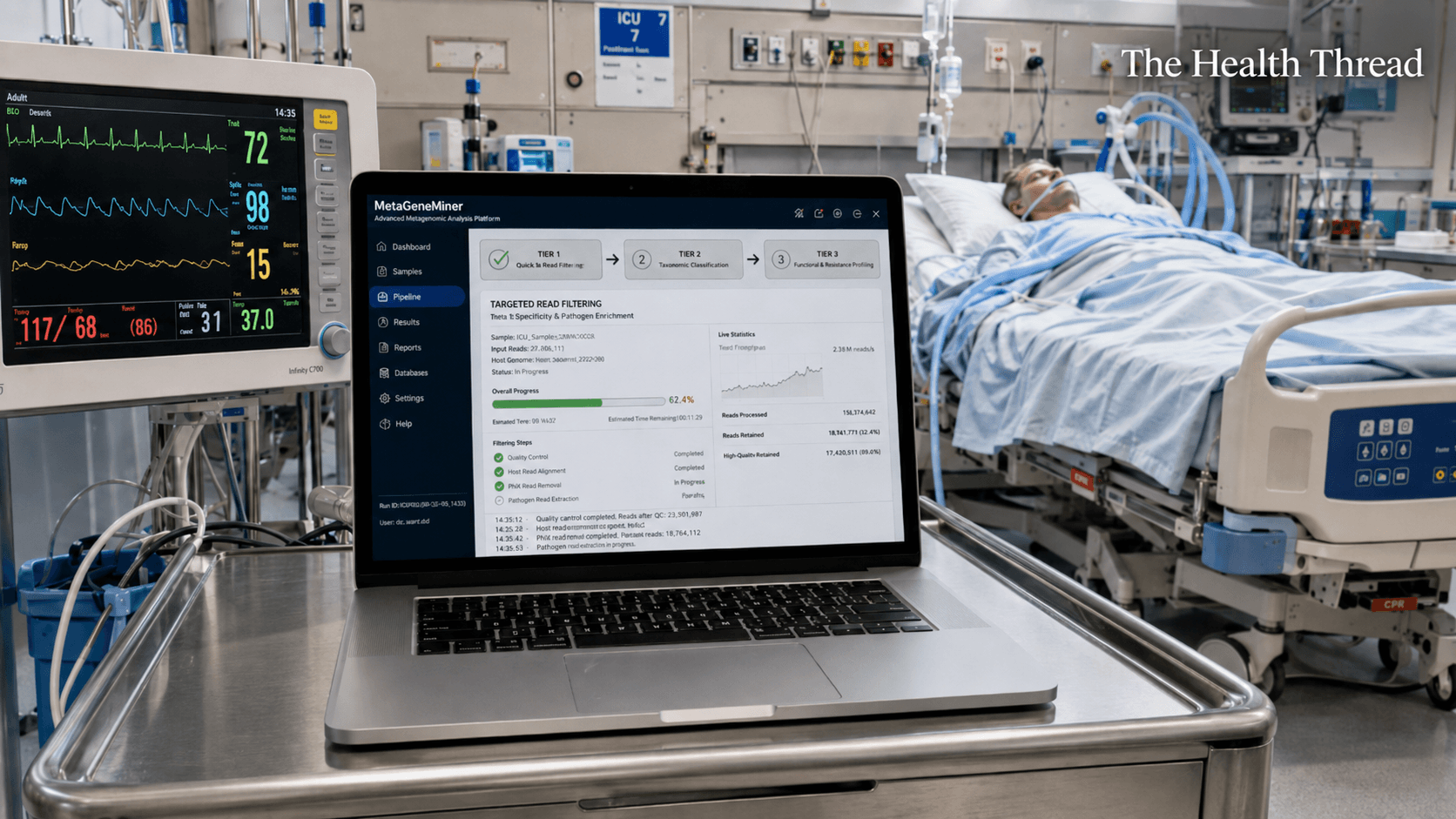
MetaGeneMiner and the High Stakes Search for Antibiotic Resistance
MetaGeneMiner: Rapid Genomic Diagnosis for Critical Care • The Challenge: Traditional antibiotic susceptibility testing is too slow for the ICU, often taking days to identify resistant "superbugs" while patients decline. • The Innovation: Researchers at Sichuan University developed MetaGeneMiner, a tool that uses a mathematical "k-mer" shortcut to extract specific resistance genes from complex DNA samples in hours. • Performance: Validated on ICU patients with A. baumannii and HSV-1, the software finished analyses in roughly two hours, nearly four times faster than standard digital mapping methods.
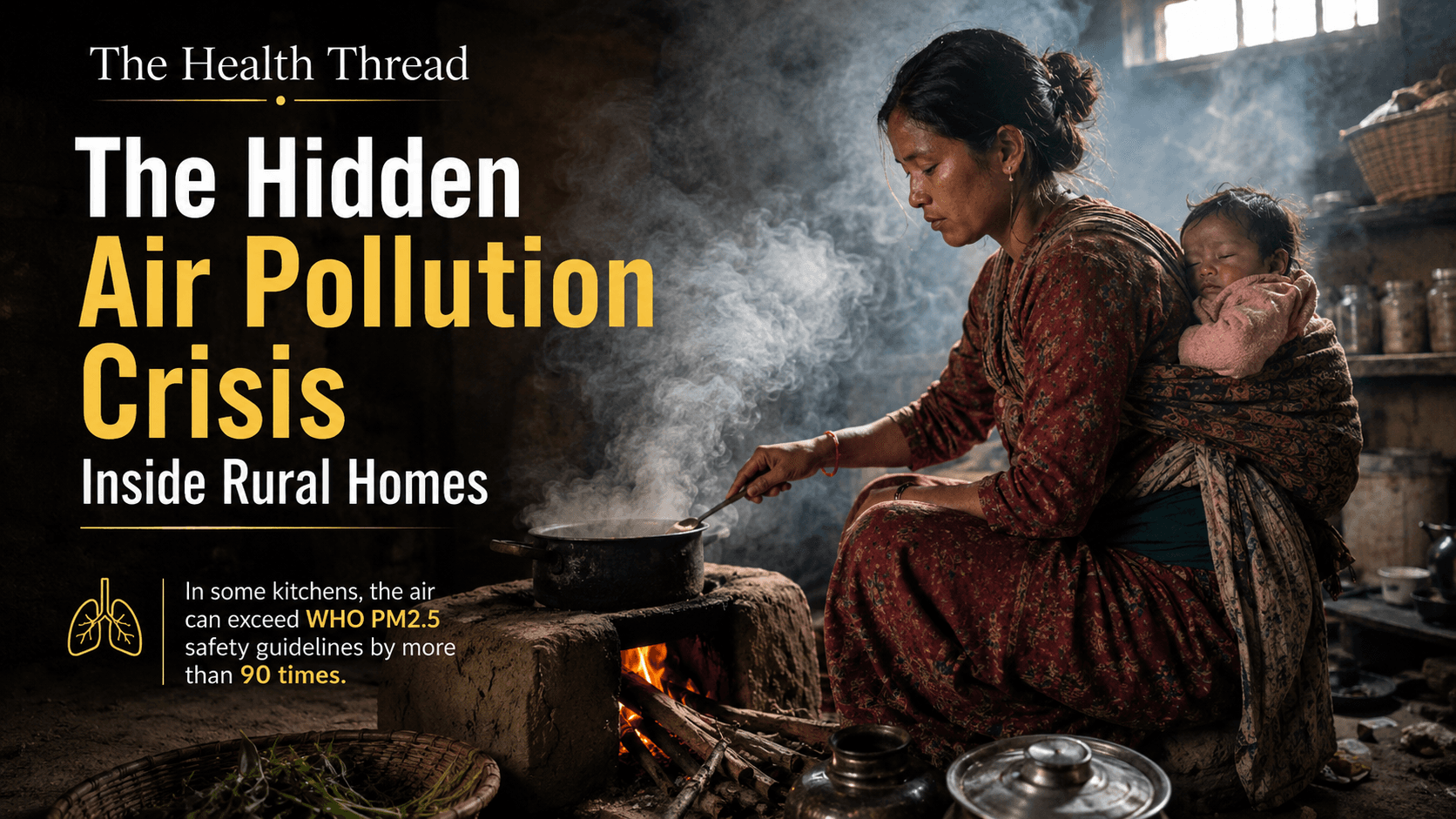
The Deadliest Room in the House: Indoor Air Pollution and South Asia's Most Overlooked Public Health Emergency
South Asia accounts for 36 percent of the world's household air pollution deaths, yet every policy conversation about "air quality" focuses on the outdoors. This investigation traces what's actually inside the smoke, from carcinogenic particulates to an overlooked contributor, incense, and asks why a woman's kitchen has never been classified as the hazardous workplace the evidence says it is.
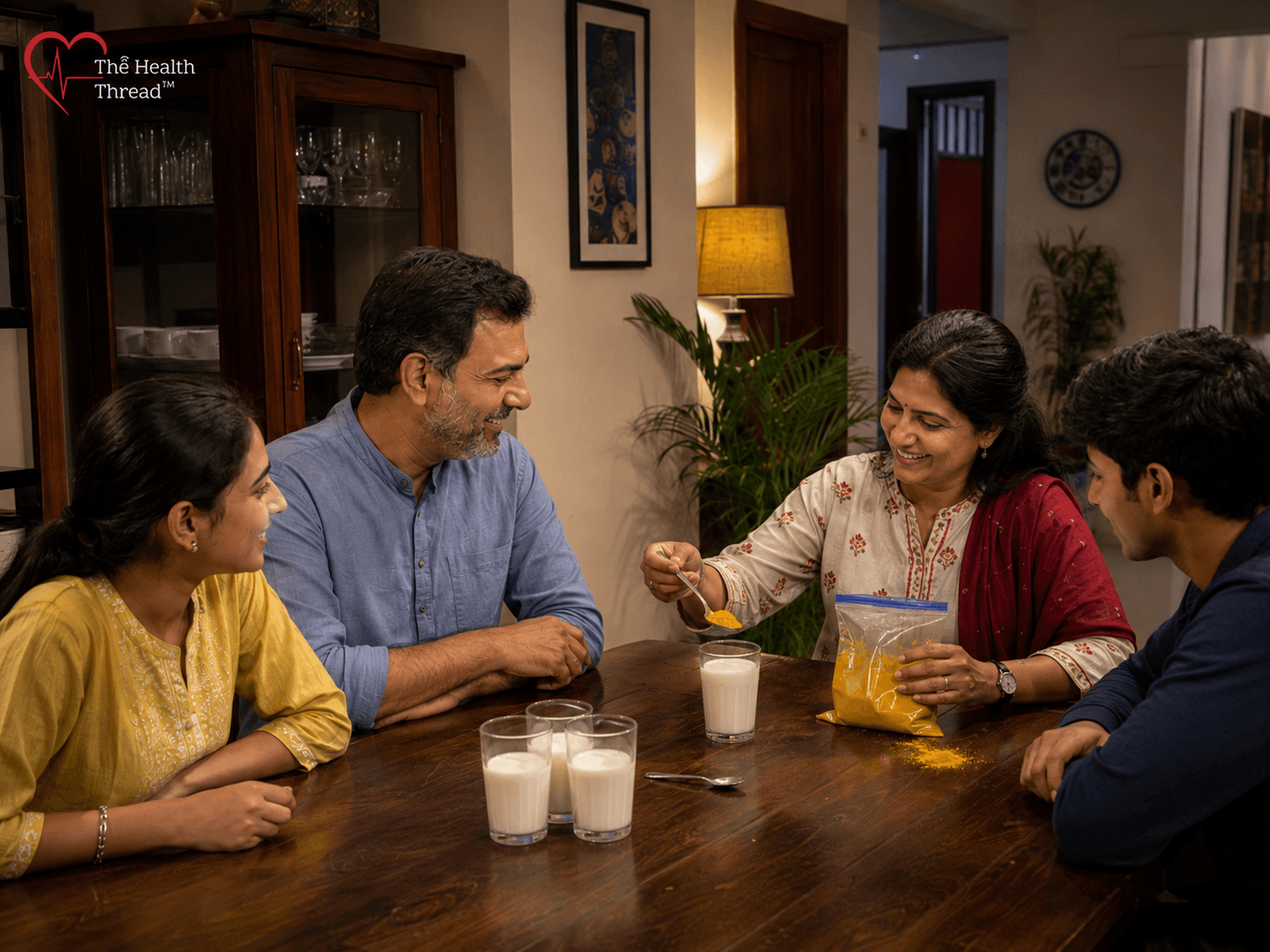
The Golden Milk Problem: What Turmeric Can and Cannot Do for You
Millions swear turmeric milk fights infection and cancer. The clinical evidence says otherwise. Curcumin, the compound responsible for turmeric's reputation, has shown real promise in laboratory studies, but human trials tell a far more modest story. No clinical trial has shown it shrinking a tumour on its own, and the strongest evidence simply doesn't support golden milk as a stand-in for medical care. The real risk isn't the drink itself. It's what happens while you're waiting for it to work. For people with active infections or undiagnosed symptoms, every week spent on a kitchen remedy instead of a doctor's visit is a week the underlying problem goes untreated, and in conditions like cancer, that delay can be the difference between early treatment and a much harder road ahead.
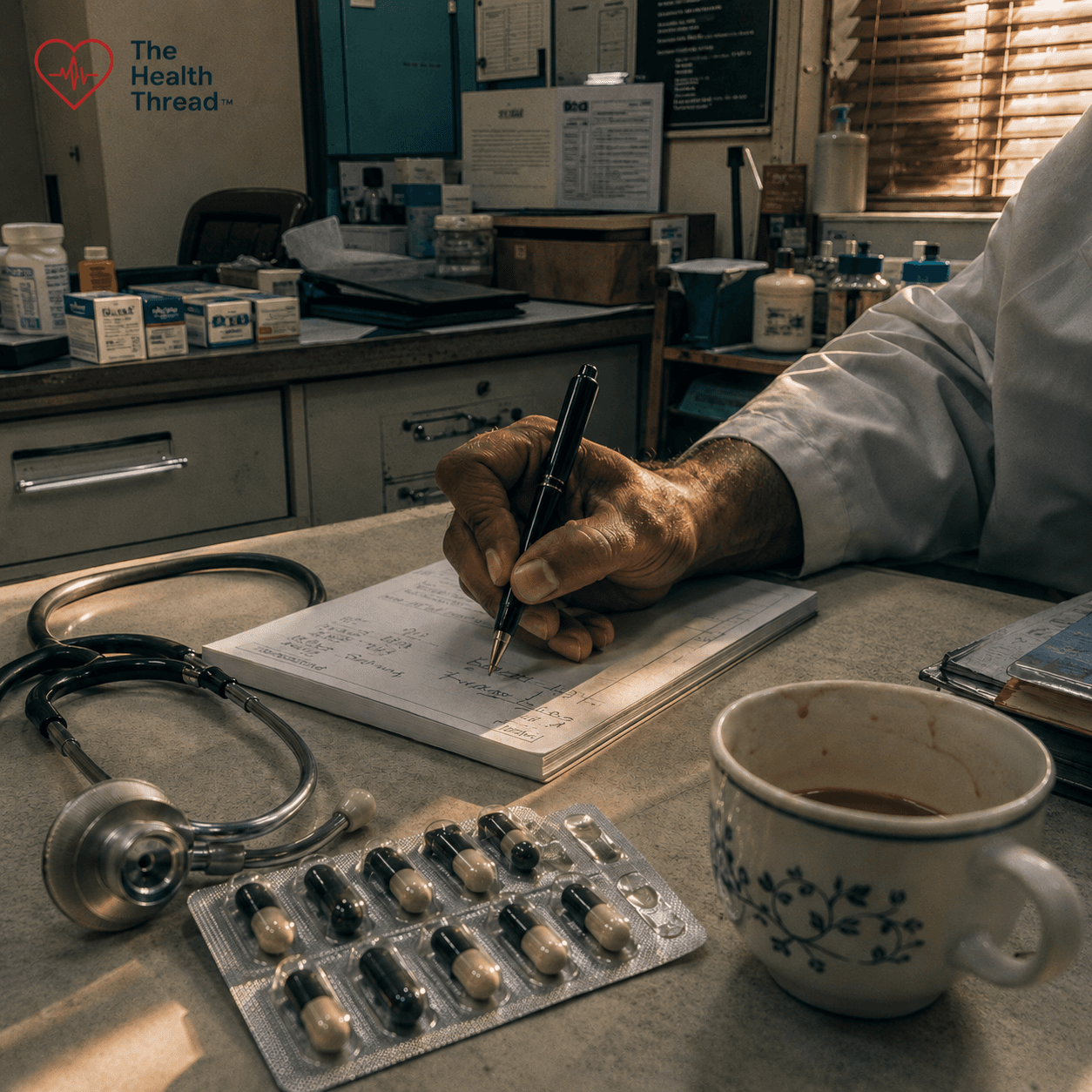
Prescribing Without Diagnosis: Antibiotic Overuse, Clinical Complicity, and the Coming Catastrophe of Antimicrobial Resistance
40-70% of all antibiotic prescriptions worldwide are written without a confirmed bacterial diagnosis. The result: 39 million preventable deaths projected by 2050. South Asia sits at the epicentre of a resistance crisis fueled by patient pressure, diagnostic uncertainty, and systems that make inappropriate prescribing the default. The post-antibiotic era isn't a metaphor; it's arriving on schedule.
Health News
See allRising above HIV diagnosis and turning pain into purpose
क्षयरोग सेवा दशकौँदेखि विस्तार भइरहँदा पनि हामी किन अझै क्षयरोग अन्त्य गर्ने बाटोमा छैनौँ?
धोएर मात्रै सफा नहुने: दक्षिण एसियाको खानामा लुकेको विषादी संकट
अफ्रिकामा लैङ्गिक समानता र स्वास्थ्य अधिकारविरुद्ध बढ्दो पितृसत्तात्मक प्रतिरोध
संयोगले होइन, नियोजित रूपमा: विश्वव्यापी संक्रामक रोग वित्तीय सहयोगमा संरचनागत असमानता
Wellness & Lifestyle
See allIn Depth
Long Reads
Policy & Public Health
Rising above HIV diagnosis and turning pain into purpose
क्षयरोग सेवा दशकौँदेखि विस्तार भइरहँदा पनि हामी किन अझै क्षयरोग अन्त्य गर्ने बाटोमा छैनौँ?
धोएर मात्रै सफा नहुने: दक्षिण एसियाको खानामा लुकेको विषादी संकट
अफ्रिकामा लैङ्गिक समानता र स्वास्थ्य अधिकारविरुद्ध बढ्दो पितृसत्तात्मक प्रतिरोध
The Deadliest Room in the House: Indoor Air Pollution and South Asia's Most Overlooked Public Health Emergency
Experts Urge Indonesia to Ratify Global Tobacco Treaty and Enforce Industry Accountability
The invisible must get served first by a legally binding treaty for older persons
Feminist Lens on AMR: Why Gender Inequality Fuels Drug Resistance
Explore Health Topics
Get The Health Thread delivered to your inbox
Join thousands of readers who start their week with our curated health news, research breakthroughs, and expert analysis. Free, every Monday.
No spam, ever. Unsubscribe anytime.
“Ethical Health Journalism, from Kathmandu to the World”
The Health Thread bridges the gap between complex medical research and everyday readers.