Nepal Health News, IPAC & Research | The Health Thread

Top Stories
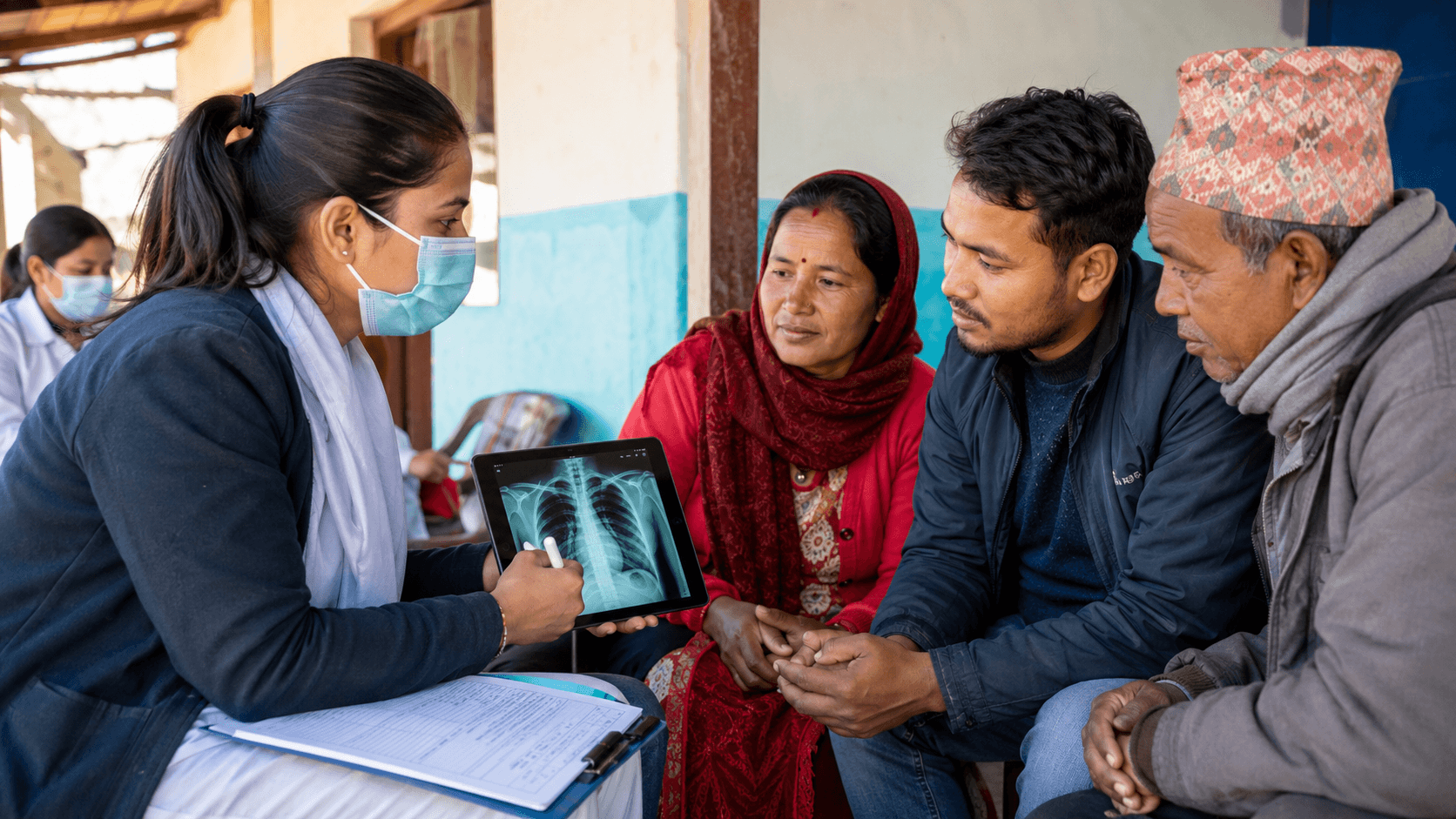
क्षयरोग सेवा दशकौँदेखि विस्तार भइरहँदा पनि हामी किन अझै क्षयरोग अन्त्य गर्ने बाटोमा छैनौँ?
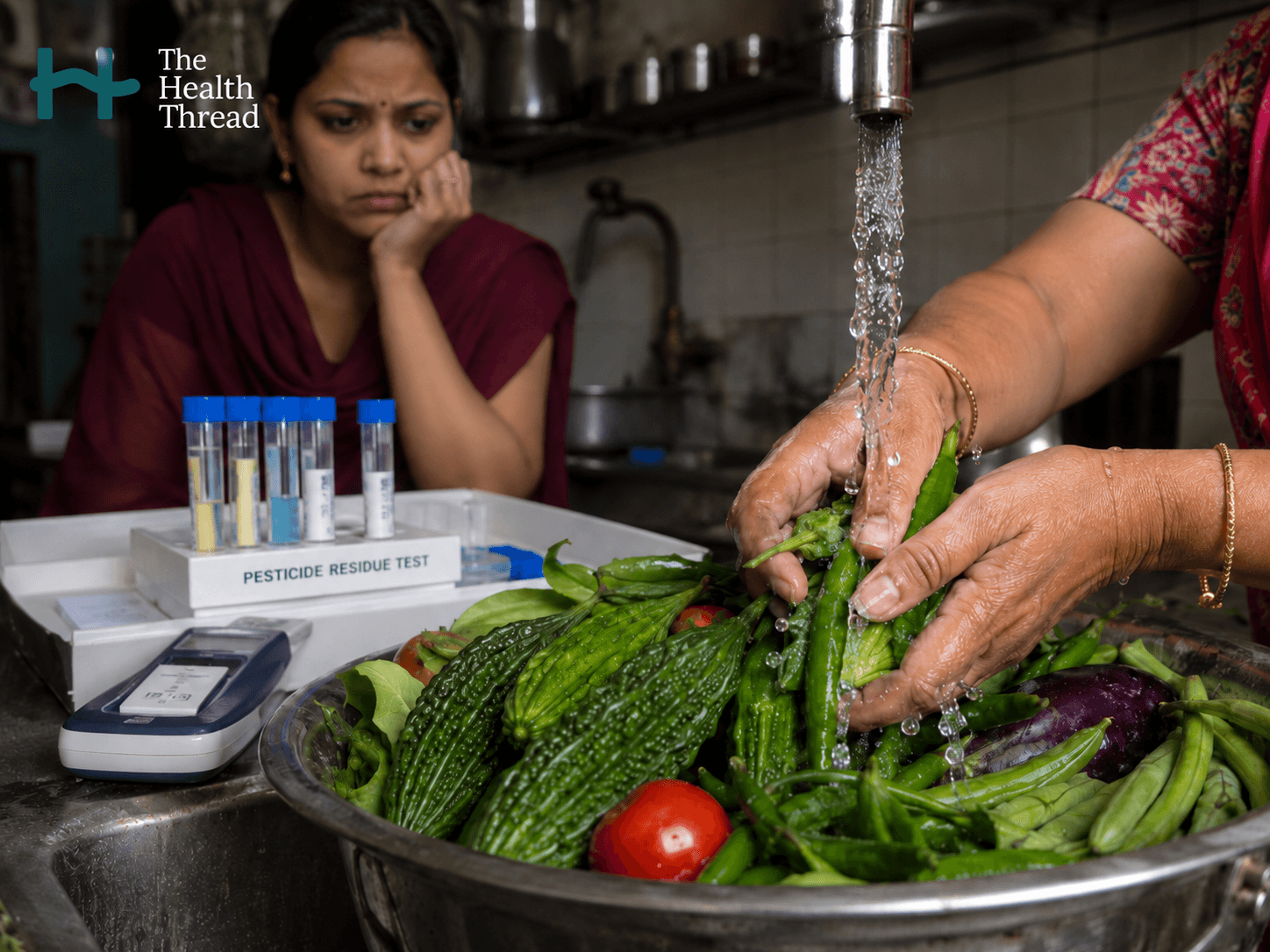
धोएर मात्रै सफा नहुने: दक्षिण एसियाको खानामा लुकेको विषादी संकट
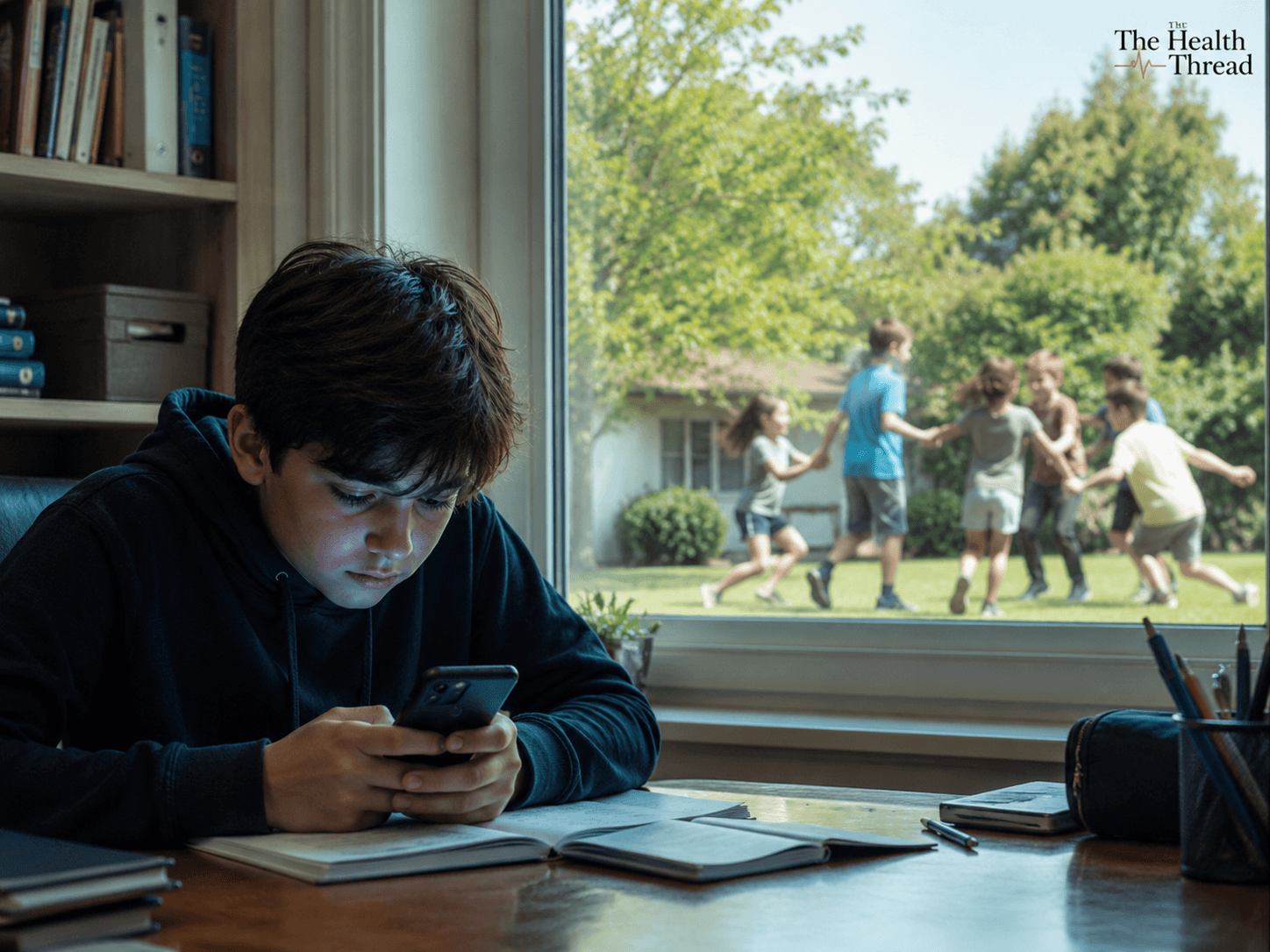
स्क्रिनले खोस्दै गएको बाल्यकाल: स्मार्टफोन, सामाजिक सञ्जाल र बालबालिकाको मानसिक स्वास्थ्य
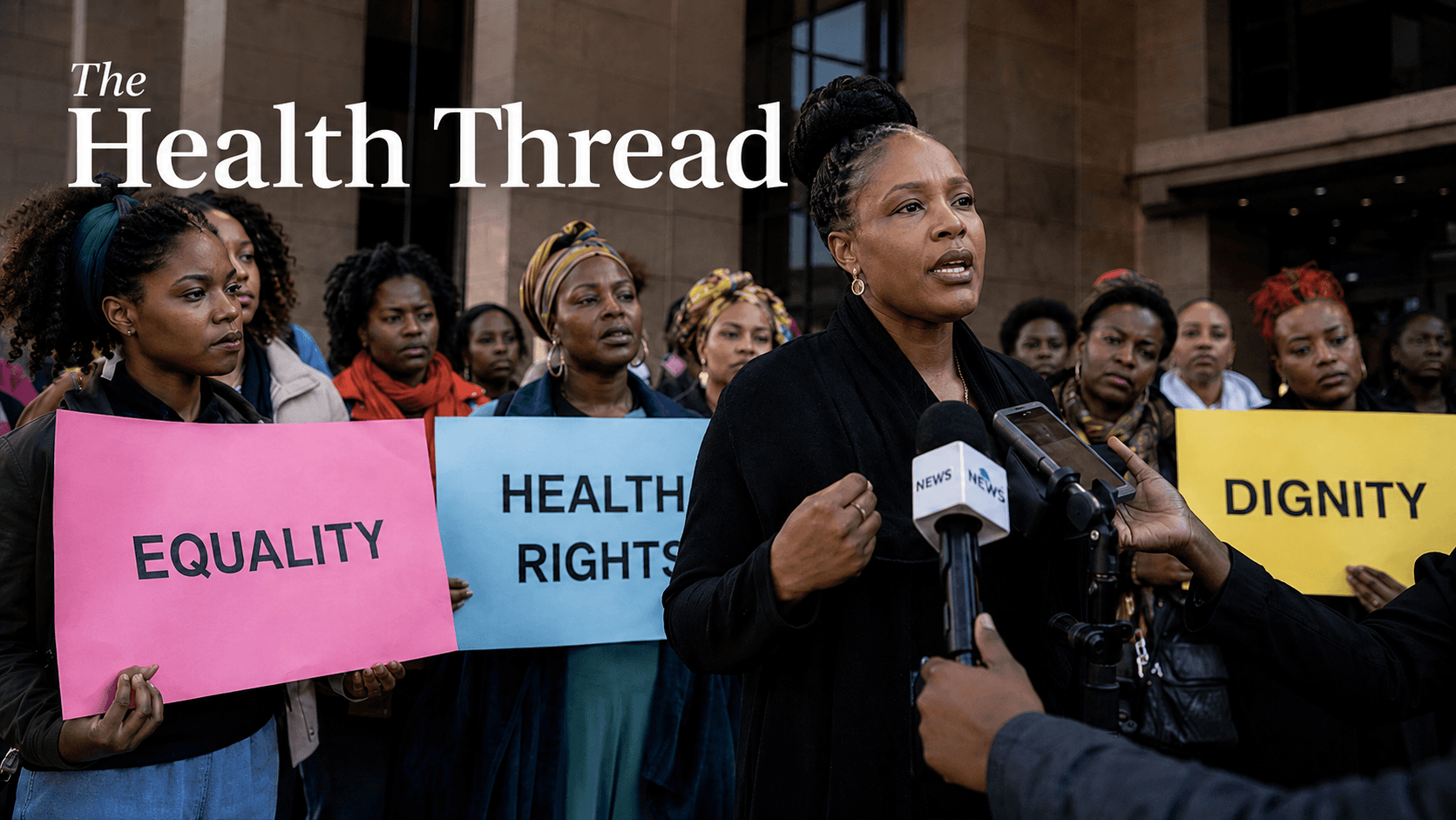
अफ्रिकामा लैङ्गिक समानता र स्वास्थ्य अधिकारविरुद्ध बढ्दो पितृसत्तात्मक प्रतिरोध
बिरामीलाई दिने जुस: पौष्टिक आहार कि फलको नाममा गुलियो भ्रम?
Your trusted source for Nepal health news, evidence-based IPAC guidelines, and the latest clinical research.
Research Watch
Latest Findings
More from Research Watch

Protecting the Smallest Lungs from the Hidden Grip of RSV in Kathmandu
Kamala Shrestha
The Heavy Burden of Bullying on Student Wellbeing in Nepal
Sabina Maharjan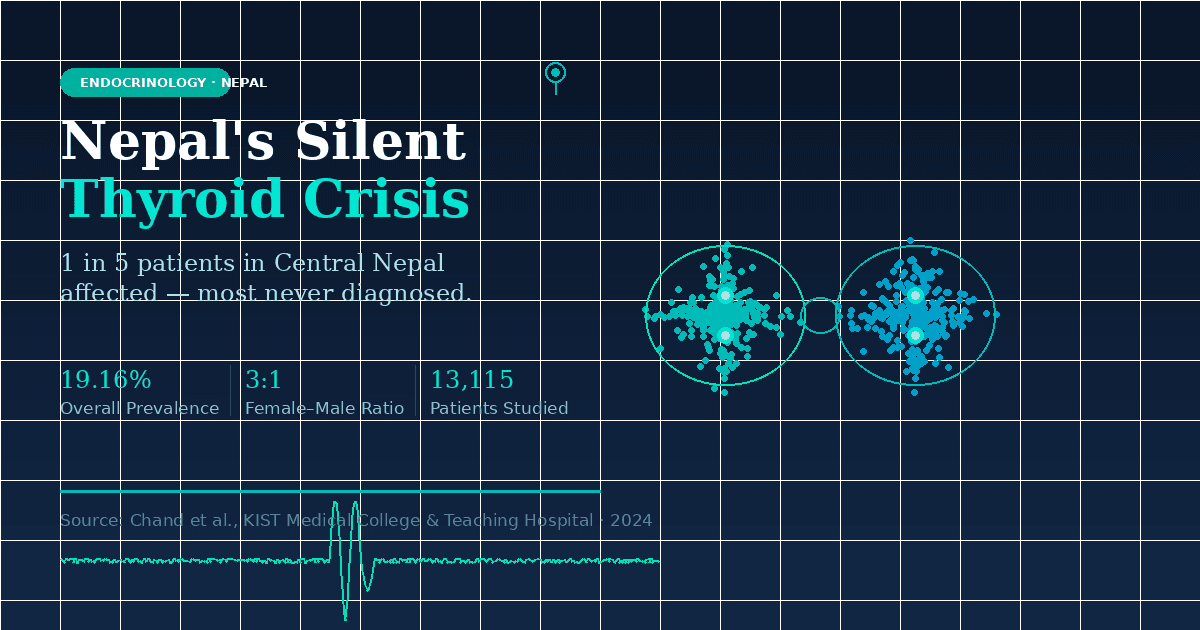
The Emerging Landscape of Thyroid Health in Central Nepal
Priya Lohani
How a Recent Western Nepal Study is Redefining Anemia Diagnosis
Anusha BastolaGlobal Health & Current Affairs
Full CoverageUnmasking the Crisis of Elder Abuse and Declining Health in Nepal
A recent study of 385 seniors in Kathmandu reveals that nearly one-third experience abuse, mostly psychological and financial, while chronic diseases like hypertension and diabetes go undertreated. Researchers are calling for urgent reform in elder care, legal protection, and geriatric health services across Nepal.
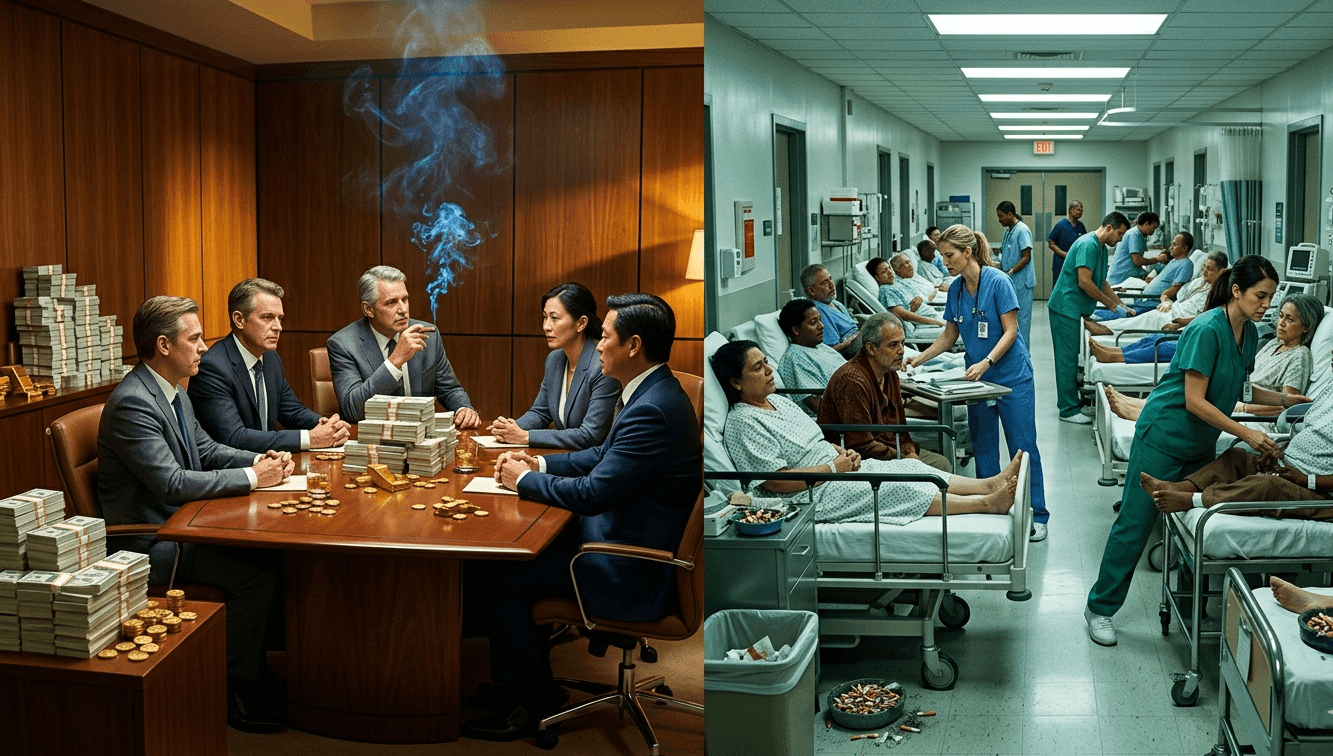
Will governments make the tobacco industry pay for all the harms it causes?
A global coalition is demanding that Big Tobacco be held financially accountable for $1.4 trillion in annual societal costs. The Make Big Tobacco Pay campaign urges governments to enforce WHO treaty obligations and ensure that the industry, not taxpayers, covers the full costs of its deadly and polluting products.
Global Healthcare Under Siege: Attacks Endanger Lives in Conflict Zones
A recent report reveals over 19,000 global attacks on healthcare since 2016, with 3,860 health workers tragically killed by 2025. Conflict-ridden nations like the Democratic Republic of Congo, Ukraine, and Sudan face relentless violence, directly impacting hospitals, medical staff, and crucial services. The increasing use of drones and explosive weapons intensifies this crisis, normalizing threats to vital medical aid and jeopardizing patient care worldwide.
Read Update →Frozen Blueberry Recall: Understanding E. coli O145 and Food Safety
Frutas y Hortalizas del Sur S.A. is recalling GreenWise Organic IQF Blueberries due to potential E. coli O145 contamination. This pathogenic bacterium can cause severe illness, including bloody diarrhea and a serious kidney complication called Hemolytic Uremic Syndrome. Consumers should discard or return the affected product and practice vigilant food hygiene to prevent infection.
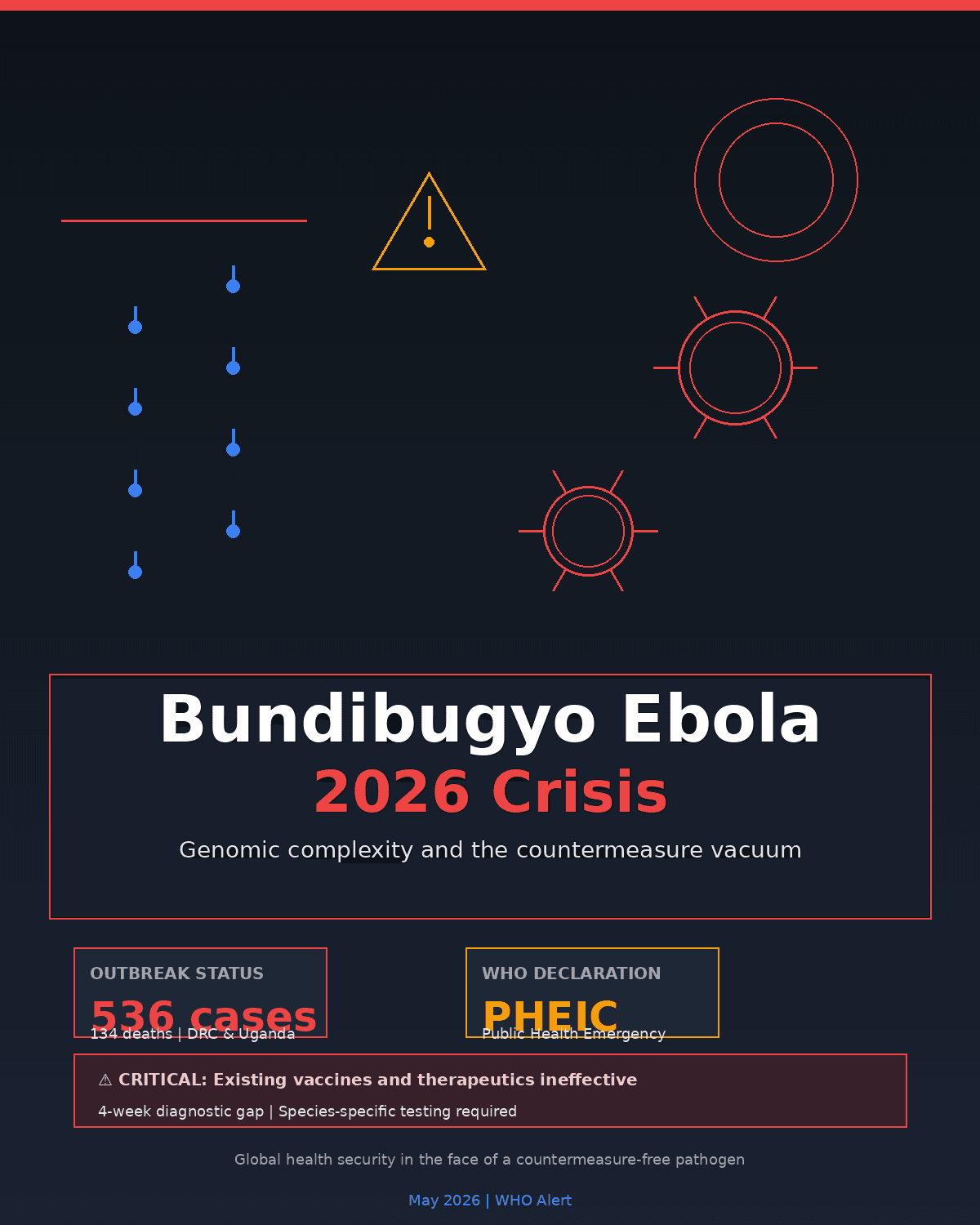
Bundibugyo Ebola Spreads: DRC Sees Rapid Increase, Uganda Stays Vigilant
Public Health Alert: Undeclared Allergen in Beef Jerky Poses Risk
African Leaders Unite in DR Congo to Combat Ebola Outbreak
Nepal Secures Anti-Rabies Vaccine Supply: A Critical Step in Public Health
Editor's Picks
संयोगले होइन, नियोजित रूपमा: विश्वव्यापी संक्रामक रोग वित्तीय सहयोगमा संरचनागत असमानता
विश्वव्यापी संक्रामक रोगको संकट केवल रोगको समस्या होइन, यो असमान स्वास्थ्य प्रणालीको परिणाम हो। HIV, क्षयरोग, उपेक्षित उष्णकटिबन्धीय रोगहरू र महामारी तयारीमा देखिएको वित्तीय कटौतीले गरिब देशहरूलाई सबैभन्दा बढी जोखिममा पारेको छ। विज्ञान, औषधि र उपचार उपलब्ध भए पनि, राजनीतिक निर्णय र असमान लगानीका कारण लाखौँ रोक्न सकिने मृत्युहरू अझै जारी छन्।
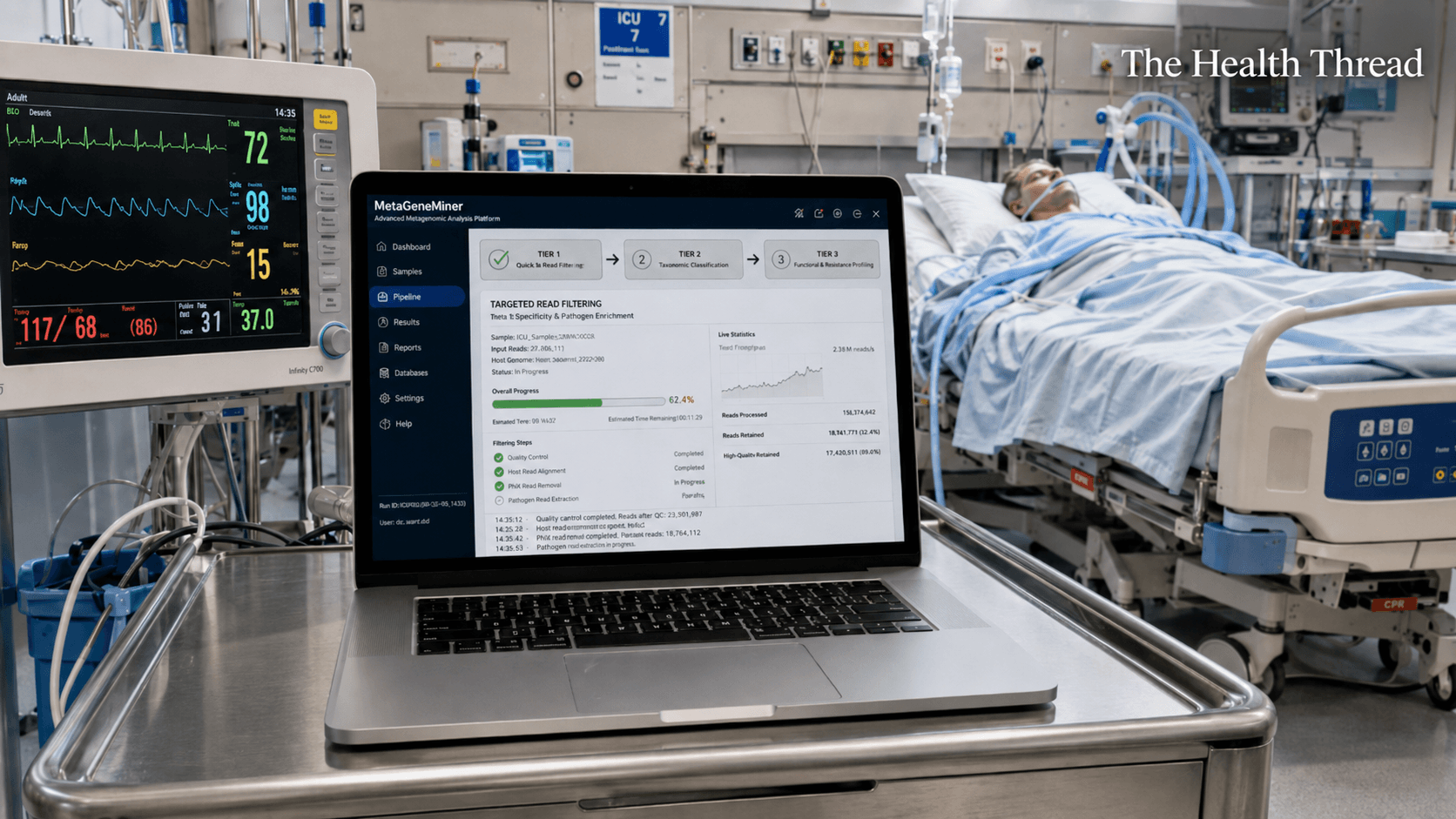
MetaGeneMiner and the High Stakes Search for Antibiotic Resistance
MetaGeneMiner: Rapid Genomic Diagnosis for Critical Care • The Challenge: Traditional antibiotic susceptibility testing is too slow for the ICU, often taking days to identify resistant "superbugs" while patients decline. • The Innovation: Researchers at Sichuan University developed MetaGeneMiner, a tool that uses a mathematical "k-mer" shortcut to extract specific resistance genes from complex DNA samples in hours. • Performance: Validated on ICU patients with A. baumannii and HSV-1, the software finished analyses in roughly two hours, nearly four times faster than standard digital mapping methods.
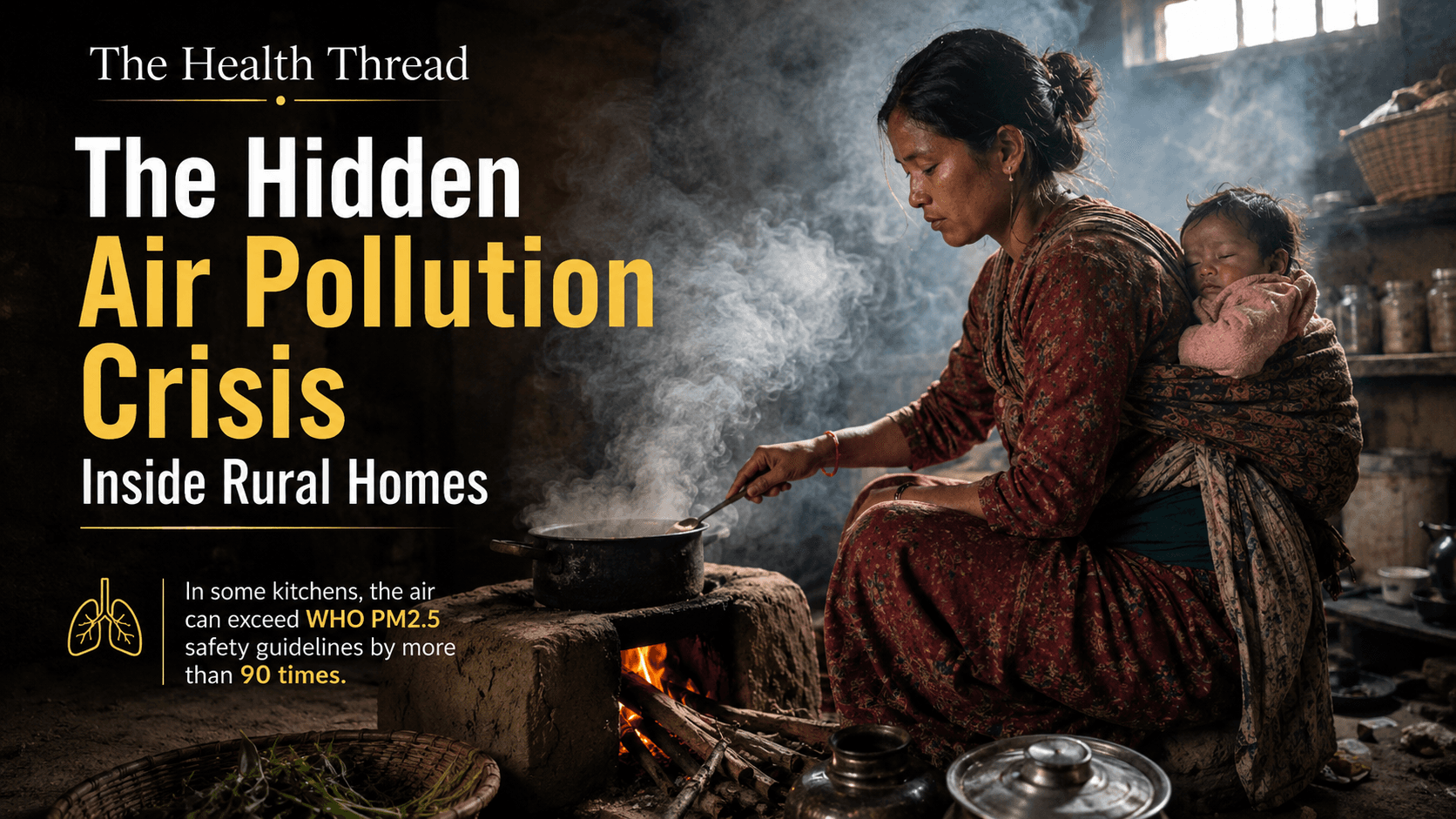
The Deadliest Room in the House: Indoor Air Pollution and South Asia's Most Overlooked Public Health Emergency
South Asia accounts for 36 percent of the world's household air pollution deaths, yet every policy conversation about "air quality" focuses on the outdoors. This investigation traces what's actually inside the smoke, from carcinogenic particulates to an overlooked contributor, incense, and asks why a woman's kitchen has never been classified as the hazardous workplace the evidence says it is.
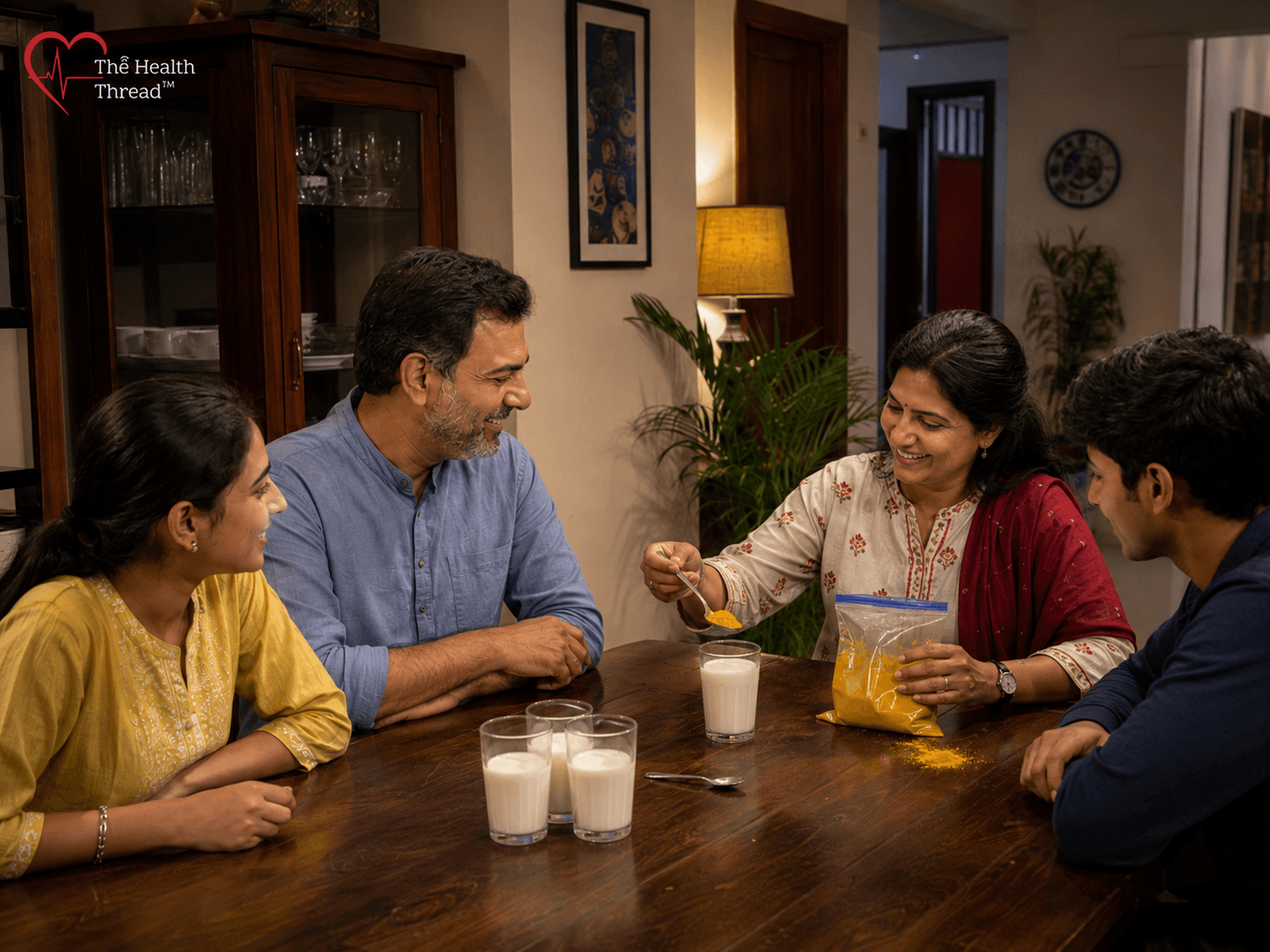
The Golden Milk Problem: What Turmeric Can and Cannot Do for You
Millions swear turmeric milk fights infection and cancer. The clinical evidence says otherwise. Curcumin, the compound responsible for turmeric's reputation, has shown real promise in laboratory studies, but human trials tell a far more modest story. No clinical trial has shown it shrinking a tumour on its own, and the strongest evidence simply doesn't support golden milk as a stand-in for medical care. The real risk isn't the drink itself. It's what happens while you're waiting for it to work. For people with active infections or undiagnosed symptoms, every week spent on a kitchen remedy instead of a doctor's visit is a week the underlying problem goes untreated, and in conditions like cancer, that delay can be the difference between early treatment and a much harder road ahead.
More Stories
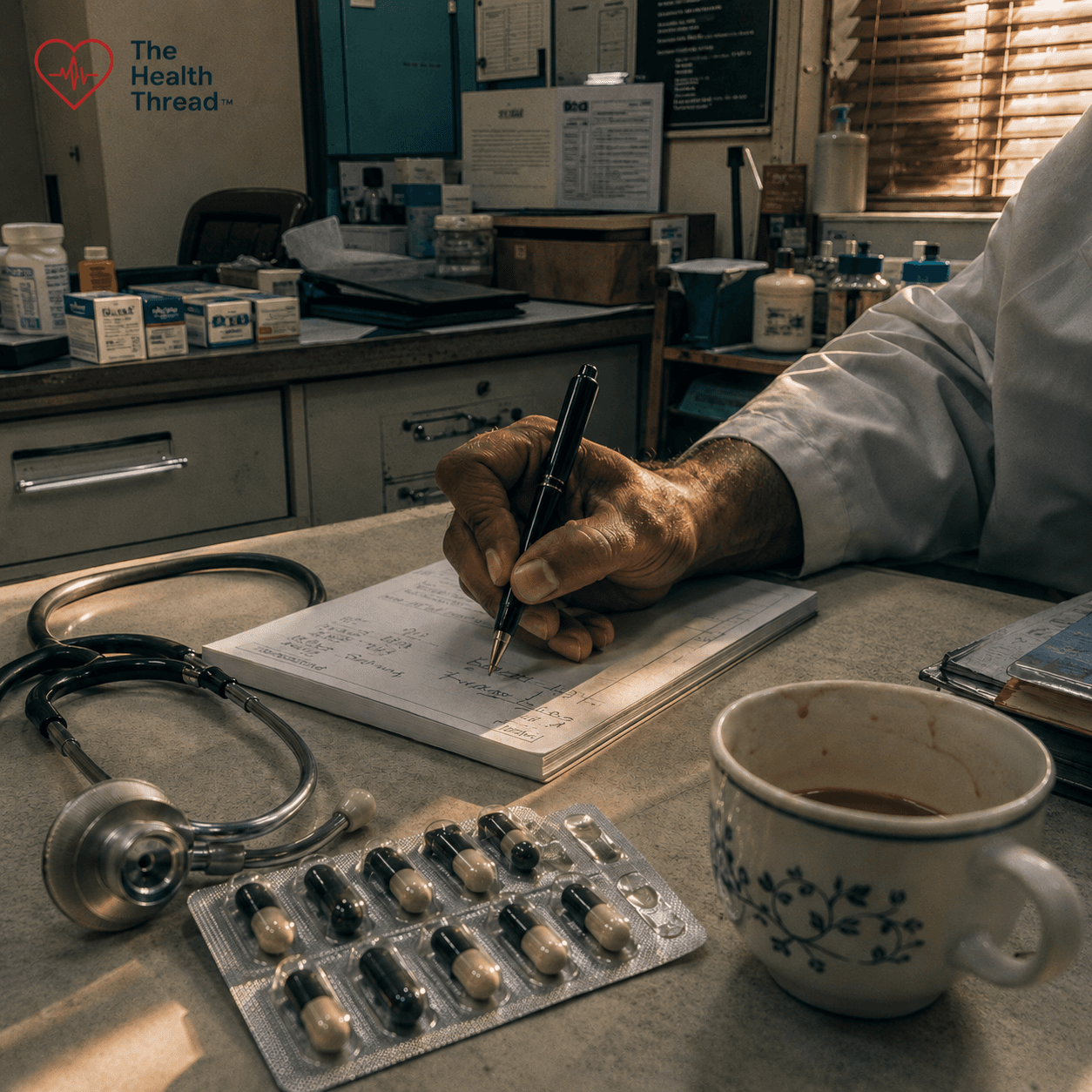
Prescribing Without Diagnosis: Antibiotic Overuse, Clinical Complicity, and the Coming Catastrophe of Antimicrobial Resistance
40-70% of all antibiotic prescriptions worldwide are written without a confirmed bacterial diagnosis. The result: 39 million preventable deaths projected by 2050. South Asia sits at the epicentre of a resistance crisis fueled by patient pressure, diagnostic uncertainty, and systems that make inappropriate prescribing the default. The post-antibiotic era isn't a metaphor; it's arriving on schedule.
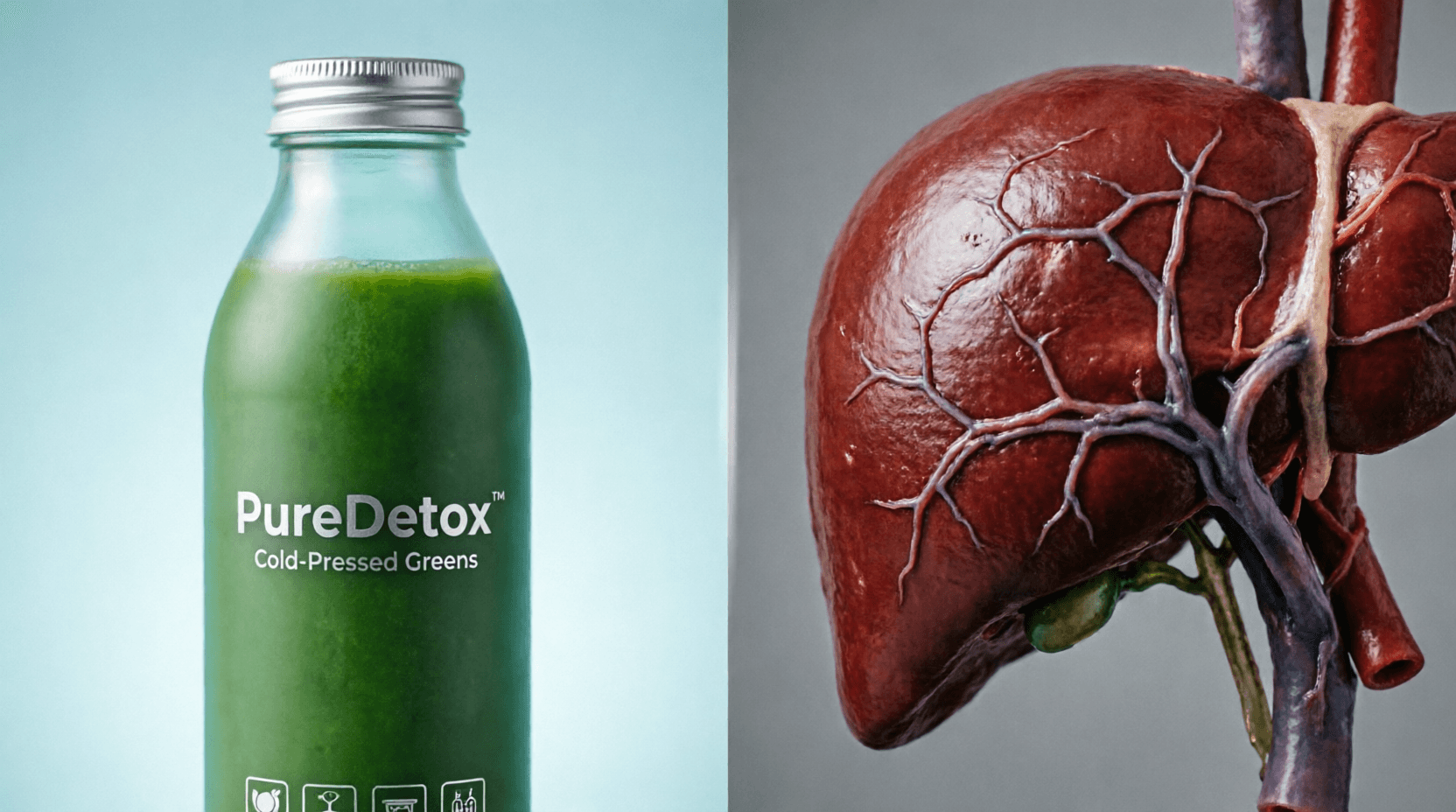
The Detox Industry and the Mythology of Liver Cleansing: A Scientific Examination
The detox industry is an $82 billion lie. Your liver detoxes itself 24/7 no juice cleanse required. Scientific evidence shows zero commercial product can enhance your body's natural detoxification, yet millions buy into the myth, while some products actually damage the liver they claim to help. This is medical misinformation at scale.

The South Asian Trap: Why Alcohol Hits Nepal Harder
A 2026 study at Nepalgunj Medical College reveals a silent epidemic of alcoholic liver disease (ALD) in Nepal, with a 14% mortality rate among 384 hospitalized patients. The research found that South Asians are genetically more susceptible to liver damage, developing ALD with less alcohol consumption than Western populations. While men in their 40s comprised 80% of cases, women faced higher death rates (17.7% vs. 13.1%). With over 77% of patients presenting with jaundice and hepatic encephalopathy causing 81% of deaths, researchers urge immediate public health interventions, including routine screening and early detection programs, to address this preventable crisis.

Unmasking the Crisis of Elder Abuse and Declining Health in Nepal
A recent study of 385 seniors in Kathmandu reveals that nearly one-third experience abuse, mostly psychological and financial, while chronic diseases like hypertension and diabetes go undertreated. Researchers are calling for urgent reform in elder care, legal protection, and geriatric health services across Nepal.
Will governments make the tobacco industry pay for all the harms it causes?
A global coalition is demanding that Big Tobacco be held financially accountable for $1.4 trillion in annual societal costs. The Make Big Tobacco Pay campaign urges governments to enforce WHO treaty obligations and ensure that the industry, not taxpayers, covers the full costs of its deadly and polluting products.
Experts Urge Indonesia to Ratify Global Tobacco Treaty and Enforce Industry Accountability
Indonesia remains one of only 8 countries yet to ratify the WHO tobacco treaty. Over 1,500 health experts are now demanding action to protect millions from a deadly, costly epidemic.
Health News
See allक्षयरोग सेवा दशकौँदेखि विस्तार भइरहँदा पनि हामी किन अझै क्षयरोग अन्त्य गर्ने बाटोमा छैनौँ?
धोएर मात्रै सफा नहुने: दक्षिण एसियाको खानामा लुकेको विषादी संकट
अफ्रिकामा लैङ्गिक समानता र स्वास्थ्य अधिकारविरुद्ध बढ्दो पितृसत्तात्मक प्रतिरोध
संयोगले होइन, नियोजित रूपमा: विश्वव्यापी संक्रामक रोग वित्तीय सहयोगमा संरचनागत असमानता
The Deadliest Room in the House: Indoor Air Pollution and South Asia's Most Overlooked Public Health Emergency
Mind, Body & Fitness
In Depth
Long Reads
Policy & Public Health
क्षयरोग सेवा दशकौँदेखि विस्तार भइरहँदा पनि हामी किन अझै क्षयरोग अन्त्य गर्ने बाटोमा छैनौँ?
धोएर मात्रै सफा नहुने: दक्षिण एसियाको खानामा लुकेको विषादी संकट
अफ्रिकामा लैङ्गिक समानता र स्वास्थ्य अधिकारविरुद्ध बढ्दो पितृसत्तात्मक प्रतिरोध
The Deadliest Room in the House: Indoor Air Pollution and South Asia's Most Overlooked Public Health Emergency
Experts Urge Indonesia to Ratify Global Tobacco Treaty and Enforce Industry Accountability
The invisible must get served first by a legally binding treaty for older persons
Feminist Lens on AMR: Why Gender Inequality Fuels Drug Resistance
Explore Health Topics
Get The Health Thread delivered to your inbox
Join thousands of readers who start their week with our curated health news, research breakthroughs, and expert analysis. Free, every Monday.
No spam, ever. Unsubscribe anytime.
“Ethical Health Journalism, from Kathmandu to the World”
The Health Thread bridges the gap between complex medical research and everyday readers.